1. Introduction
Liver fibrosis, characterized by the excessive accumulation of extracellular matrix proteins, is a hallmark of chronic liver diseases. The fibrogenic reaction results from repeated liver injury, the wound-healing response to such ongoing injury, and ultimately disrupts normal liver architecture and hepatic function [
1]. Over time, liver fibrosis can advance to more severe stages such as cirrhosis, predisposing to liver failure, and hepatocellular carcinoma (HCC) development, all of which significantly worsen patient outcomes [
2]. Recent research has expanded our understanding of liver fibrosis, revealing that its implications extend beyond liver-specific complications. Fibrosis is now recognized as a prognostic factor for a range of extra-hepatic conditions, including sarcopenia [
3,
4,
5,
6], cardiovascular disease (CVD) [
7,
8,
9,
10,
11,
12,
13,
14], chronic kidney disease CKD) [
15,
16,
17,
18], and even cognitive decline [
19], underscoring its systemic impact in broader health contexts.
A recent meta-analysis pinpoints that advanced liver fibrosis and cirrhosis are highly prevalent in the general worldwide population, with major geographic discrepancies. The prevalence rates are 3.3% (95% CI: 2.4–4.2) for advanced liver fibrosis and 1.3% (95% CI: 0.9–1.7) for cirrhosis, with a trend indicating an increase in prevalence after 2016 [
20]. Male sex, viral hepatitis, diabetes, excessive alcohol intake, and obesity are the main risk factors for cirrhosis [
20]. Sex differences are a critical modifier of the development, progression, and outcomes of liver fibrosis [
21]. Studies demonstrate that men and women exhibit different susceptibility to liver fibrosis [
22]. However, the relationship between sex and liver fibrosis is complex and multifaceted and modulated by hormonal, genetic, as well as environmental factors [
21]. For example, estrogen has a protective effect against fibrosis progression [
23,
24], potentially explaining the slower fibrosis rates observed in premenopausal women compared to men [
25]. Additionally, sex differences in immune responses [
26], fat distribution [
27], and metabolic processes [
28] also contribute to disparities in the risk of liver fibrosis development ad progression among men and women.
In this review, we aim to summarize the current understanding of the pathomechanisms underlying sex and gender differences in liver fibrosis. We will also explore how these differences influence both intra- and extra-hepatic complications. By highlighting these differences, we hope to provide insights that could lead to more personalized strategies for managing liver fibrosis in both men and women.
2. Pathomechanisms Contributing to Sex Differences in Liver Fibrosis
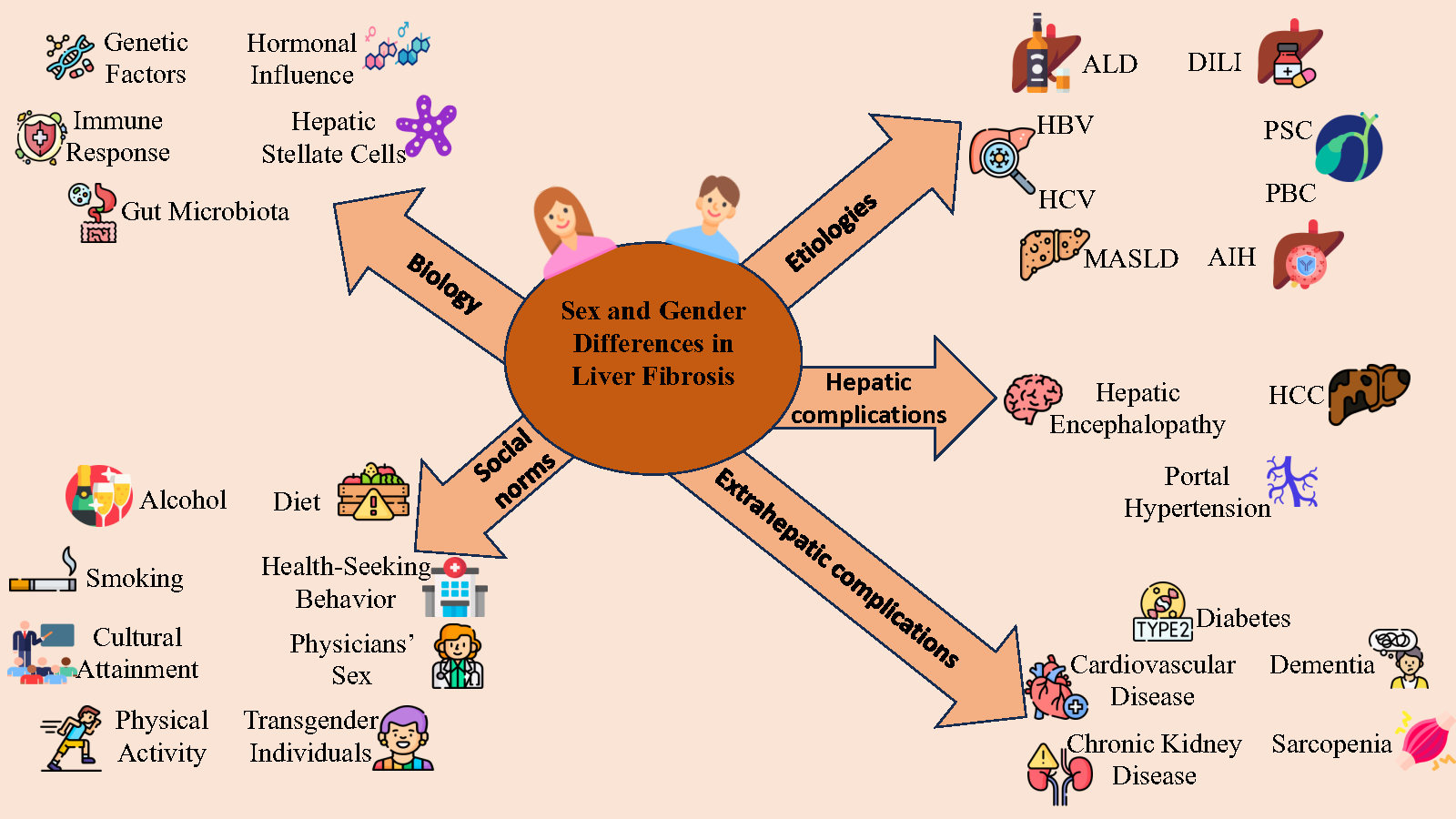
Sex differences in the prevalence, severity, and outcomes of liver fibrosis are well-documented. Understanding these differences is crucial for developing sex-specific therapeutic interventions and improving outcomes in patients with liver disease. Various factors contribute to sex differences in liver fibrosis, including genetics, hormonal influences, immune system responses, and lifestyle factors (). Research shows that females generally have a lower risk of liver fibrosis compared to males, particularly in conditions such as chronic hepatitis C and nonalcoholic fatty liver disease (NAFLD) [
29,
30], now renamed metabolic dysfunction-associated steatotic liver disease (MASLD). This susceptibility varies across different stages of reproductive life, including puberty, pregnancy, and menopause, highlighting the importance of considering sex differences in liver disease management [
21].
. Factors contributing to sex differences in liver fibrosis *.
Genomic studies have identified several sex-limited genes that influence liver fibrosis [
57]. For example, a male-specific Y chromosome gene sex-determining region Y (SRY) is linked to fibrogenesis and can affect hepatic stellate cell (HSC) activation and fibrosis progression. This was demonstrated in hepatocyte-specific
Sry knock-in mice that developed exacerbated liver fibrosis, whereas
Sry knockout mice had alleviated liver fibrosis when subjected to bile duct ligation for 2 weeks or carbon tetrachloride treatment [
31]. Mechanistically, it was suggested that the SRY expression in hepatocytes can transcriptionally regulate
Pdgfrα expression and promote high mobility group box 1 release, which are key factors in the activation of HSCs and transdifferentiation into myofibroblasts [
32].
Conversely, females benefit from X-linked genes that promote protective pathways. The X-linked inhibitor of apoptosis (XIAP), for instance, plays a key role in liver maintenance, and its loss can trigger liver diseases, underscoring its importance under normal physiological conditions [
58]. It is well accepted that XIAP is a potent anti-apoptotic protein that can physically interact and block the enzymatic activities of various caspases, thereby inhibiting both the extrinsic and intrinsic apoptotic pathways [
59,
60]. In the same line, the absence of XIAP has been shown to sensitize cells and mice to lipopolysaccharide and TNF-mediated cell death. Mice lacking XIAP are more susceptible to liver damage than wildtype mice [
61].
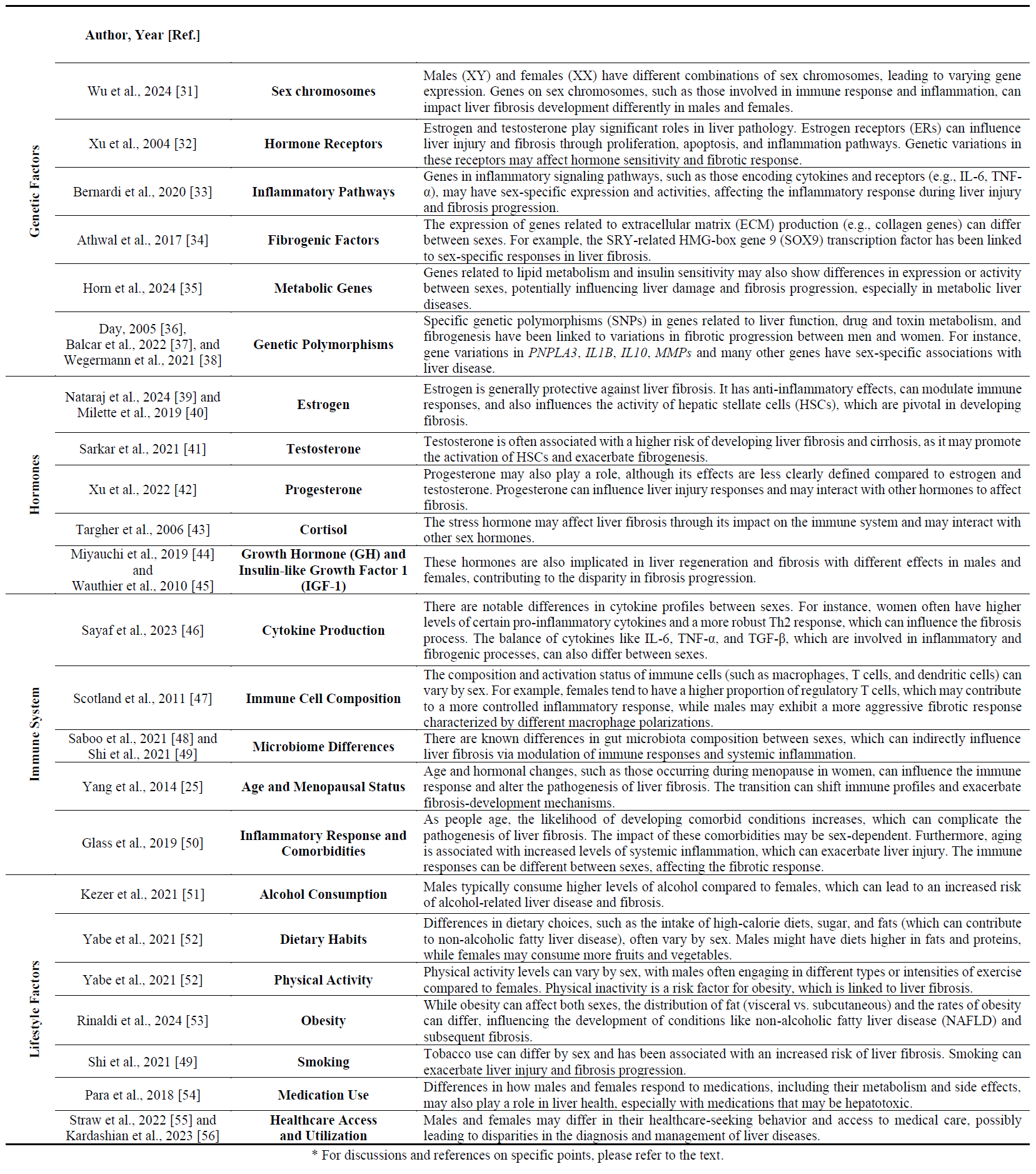
2.2. Hormonal Influence
Hormones such as estrogens, progesterone, androgens (such as testosterone), cortisol, growth hormone, and insulin-like growth factor (IGF) significantly impact liver metabolism and pathobiology by influencing immune responses, inflammation, and fibrogenesis (). Estrogen is known for its anti-fibrogenic properties, occurring via inhibition of HSC activation and extracellular matrix (ECM) deposition. Estrogen receptors (ERs), especially ERα, reduce fibrosis by decreasing collagen synthesis and increasing collagenase activity [
32]. On the other hand, androgens may have a pro-fibrogenic effect, potentially worsening liver fibrosis in males. Therefore, hormonal balance is crucial in disease progression [
62].
Cortisol, a stress hormone, also impacts liver fibrosis by modulating immune responses and interacting with other sex hormones. Male mice exhibit more severe insulin resistance than female mice when exposed to high cortisol levels, while female mice show more protective metabolic adaptations in adipose tissue [
63]. Similarly, growth hormone and IGF have sex-specific effects, influencing fibrosis progression by regulating liver regeneration [
64].
. Hormones contributing to sex differences in the pathogenesis of liver fibrosis. Legend to . The sex hormones estradiol, testosterone, and progesterone, along with hydrocortisone (cortisol) and the cytokines growth hormone and insulin-like growth factor-1 (IGF-1), significantly contribute to sex differences in the pathogenesis of liver fibrosis. This figure illustrates that the molecular drivers contributing to sex differences in the pathogenesis of liver fibrosis can vary from a biochemical standpoint and can include hormones or proteinogenic factors. Structures depicted were generated with Jmol (version 14.2._2015.07.09), and chemical depiction information sourced from the PubChem Compound Database [
65]. The structures for growth hormone and insulin-like growth factor (IGF) were drawn with Ribbons XP software (version 3.0) using the coordinates 1GZZ and 4HGU deposited in the RCSB Protein Data Bank [
66].
Research shows that innate and adaptive immune responses differ between men and women, with females typically exhibiting a more robust immune response [
67]. This enhanced immune activity can lead to more effective pathogen clearance but also predisposes women to autoimmune hepatic disorders. In the context of liver fibrosis, the imbalance in cytokine production is crucial. Males typically have higher levels of pro-inflammatory cytokines (e.g., IL-1β, IL-6, and TNF-α) compared to females [
33]. These elevated cytokines promote inflammation and, ultimately, fibrosis during liver injury.
2.4. Sex Differences in the Activation and Function of HSC and Extracellular Matrix Remodeling
In a CCl
4-induced liver injury mouse model, testosterone significantly influences liver injury by regulating the NLRP3 inflammasome activation-mediated inflammatory response [
68]. In contrast, estrogens reduce HSC activation, mitigating the fibrogenic response in females [
69]. Receptor and ligand expression involved in HSC activation also differ by sex. Female and male mice display different estrogen receptor expressions in HSCs, influencing fibrogenic responses [
70]. Furthermore, studies identify sex differences in the expression and activation of the transforming growth factor-β (TGF-β) pathway, a key mediator in fibrosis. For example, female mice show lower TGF-β expression than males in the CCl
4-induced liver injury model [
46].
Fibroblasts and HSCs produce collagens (types I, III, and IV) and glycoproteins that constitute the ECM. Sex-dependent variations in ECM production are evident, with females demonstrating considerably lower levels of collagen deposition in response to liver injury than males [
46]. Sex hormones also affect matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinases (TIMPs), which regulate ECM remodeling. Males tend to have lower MMP levels, leading to excessive fibrosis, while females typically have a higher MMP/TIMP ratio, indicating a more balanced fibrotic response [
46].
2.5. Microbiota Influences on Liver Fibrosis
The composition of gut microbiota affects the progression of liver fibrosis, with differences in microbial diversity and abundance based on sex. Emerging evidence links sex-dimorphic gut microbiota and bile acid profiles to different immune responses in the liver [
71]. Males tend to have a higher abundance of certain bacteria associated with increased inflammation, thereby contributing to more severe fibrosis [
72]. In contrast, females often exhibit more varied gut microbiota associated with anti-inflammatory markers, potentially offering protection against liver damage [
72]. Additionally, gut dysbiosis can trigger systemic inflammation, further promoting liver fibrosis via elevated levels of gut-derived bacterial translocation, which fuels inflammation and fibrogenesis [
73]. Studies in mice show that modifying gut microbiota through diet, probiotics, or antibiotic therapy can effectively reduce or worsen liver fibrosis. This underscores the importance of the gut-liver axis in understanding and addressing gender-related disparities in fibrosing liver disease [
74].
2.6. Future Directions and Conclusion
Future research should focus on elucidating the biological mechanisms behind sex disparities in liver disease. Investigating the roles of sex chromosomes in gene expression patterns related to fibrosis may provide new therapeutic targets [
31]. Clinical studies should also incorporate sex stratification to improve understanding of liver disease outcomes. Potential therapies could involve sex hormone modulation, such as exploring estrogen-based treatments to prevent or treat liver fibrosis in at-risk individuals. Furthermore, targeting gut microbiota through dietary interventions or probiotics may offer a novel approach to reducing fibrosis, particularly in male patients.
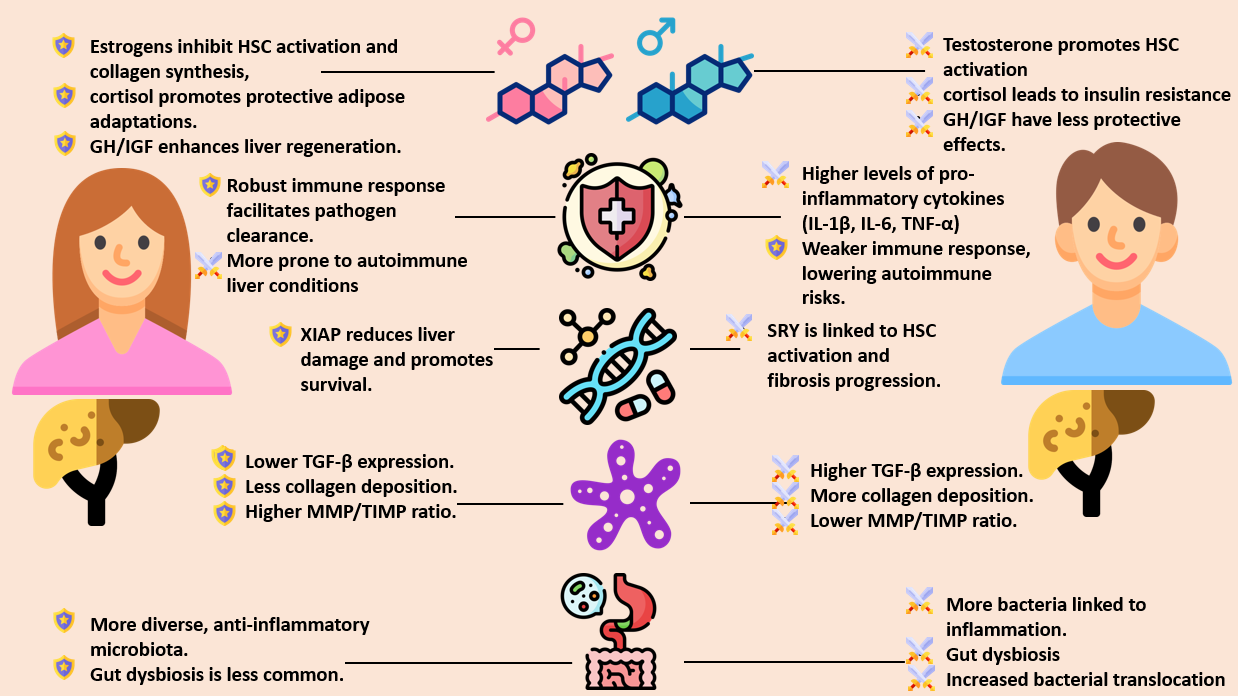
The complex interaction of genetic, hormonal, immune, and environmental factors drives sex differences in liver fibrosis. summarizes the protective and harmful pathomechanisms underlying these differences between males and females. Understanding these pathomechanisms is essential for developing targeted interventions and improving clinical outcomes in patients with liver disease. Future research must continue to uncover the intricate details of these mechanisms to create personalized treatments that address the unique needs of male and female patients. This knowledge is crucial for developing sex-specific therapies for liver diseases like cirrhosis and fibrosis, as well as for designing preventive strategies.
. Comparative summary of protective and harmful pathomechanisms underlying sex differences in liver fibrosis. Legend to . Based on references in the text, summarizes the most well-characterized hormonal, immune, genetic, and gut-liver axis-related mechanisms involved in sex and gender-disparities in liver fibrosis. The sword icon represents harmful pathomechanisms, and the shield icon represents protective ones. HSC—Hepatic stellate cell; GH—Growth hormone; IGF—Insulin-like growth factor; XIAP—X-linked inhibitor of apoptosis; TGF-β—Transforming growth factor-beta; MMP—Matrix metalloproteinase; TIMP—Tissue inhibitor of metalloproteinase; IL—Interleukin; TNF-α—Tumor necrosis factor-alpha.
3. Role of Gender
While sex is a binary biological variable, gender refers to social norms that shape roles, expectations, opportunities, and the distribution of power for women and men, and it is more fluid throughout a person’s lifetime [
75,
76]. Importantly, gender identity may differ from biological sex, as seen in transgender individuals, who may have been under-represented in medical studies [
77]. Gender is just as important as biological sex in its impact on health, influencing both patients and healthcare providers [
78]. For example, gender affects health maintenance and susceptibility to liver disease through behaviors such as diet, smoking, and physical activity (cf. ), which can alter gene expression and clinical phenotype via epigenetic modifications [
79,
80]. Typically, men are more likely to engage in risky behaviors such as excessive alcohol consumption and smoking, increasing the risk of liver fibrosis [
81]. In addition, gender plays a key role in access to preventive healthcare, acceptance of invasive diagnostic and therapeutic strategies, and overall utilzation of healthcare services [
82,
83].
Given the complexity of this topic—intertwined with race, ethnicity, historical determinants, and shifting political attitudes—in this section, we will explore well-characterized examples of how gender may affect liver fibrosis.
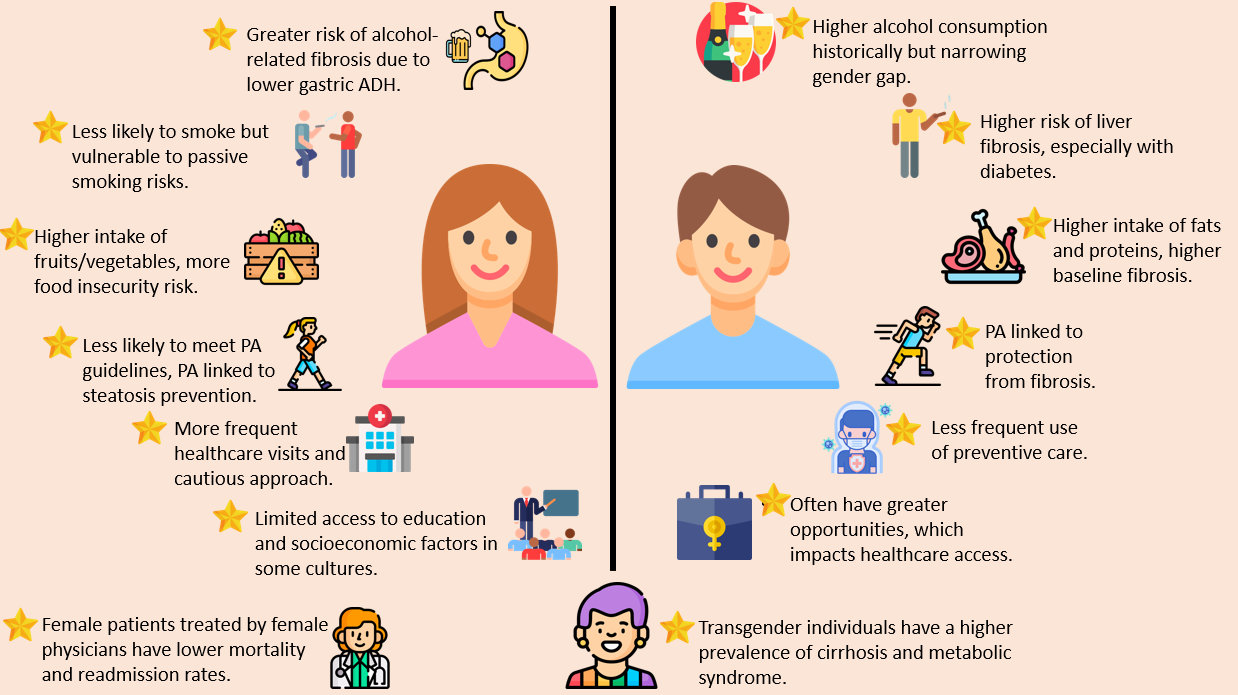
summarizes the gender differences in liver fibrosis. However, the full picture is still evolving, and more research is needed to better understand how sex and gender impact liver fibrosis.
. Comparative summary of gender differences in liver fibrosis. PA—Physical activity; ADH—alcohol dehydrogenase. Legend to . Based on the references discussed below, the cartoon illustrates the varying impact that alcohol consumption, physical activity, diet, socio-economic status, and hormonal therapies may have on liver fibrosis.
A robust body of research indicates that women are at a higher risk of alcohol-related liver fibrosis compared to men [
84]. This difference is partly due to variations in enzymatic activity. Men have 70–80% higher gastric alcohol dehydrogenase (ADH) activity, which plays a role in initial alcohol metabolism, while women exhibit higher hepatic ADH activity [
85]. Alcohol use disorder (AUD) affects approximately one in three individuals in the United States during their lifetime [
86]. While men have traditionally been more impacted by AUD, recent data shows that the gender gap has significantly narrowed due to a concerning rise in AUD prevalence among women. This undersocres the urgent need for preventive measures to address the long-term impact of alcohol on liver health [
87].
3.2. Smoking of Tobacco
Men may be at a higher risk of developing liver fibrosis and HCC due to tobacco use [
88]. Additionally, tobacco use can worsen the risk of liver fibrosis in individuals with MASLD and diabetes, suggesting that those with diabetes should consider quitting smoking [
89]. A recent study found that cotinine, a biomarker of tobacco exposure, is associated with liver fibrosis in adolescents [
90]. This highlights the importance of implementing strict laws to prevent both active and passive smoking in order to decrease the risk of liver fibrosis.
3.3. Diet
Dietary differences, such as the consumption of high-calorie diets, sugar, and fats—factors that contribute to MASLD—often vary by gender [
91]. Men typically consume higher amounts of fats and proteins, while women tend to eat more fruits and vegetables [
92]. These differences in diet lead to variations in antigen exposure and micronutrient intake, contributing to different immune aging trajectories and longevity-associated outcomes [
93]. Poor diet interacts with alcohol consumption, making individuals more susceptible to severe ALD [
94]. This is particularly relevant given that food insecurity—an emerging risk factor for developing fibrotic liver disease, irrespective of HIV status [
95,
96]—is more common among women [
97].
Additionally, gender may influence treatment response. For instance, in the case of the very low-calorie ketogenic diet (VLCKD), men tend to have higher baseline levels of steatosis and fibrosis than women, and these differences persist even after following the diet [
53].
3.4. Physical Activity
Physical activity (PA) plays a key role in determining the risk of developing MASLD and HCC [
98,
99]. PA levels typically vary between sexes, with men often engaging in different types or intensities of exercise compared to women [
100]. Physical inactivity, a risk factor for obesity, is closely linked to liver fibrosis [
101], and women are less likely to meet the PA guidelines [
102].
A cross-sectional study of 5,933 US adults reported that leisure-time PA is negatively associated with steatosis in women and individuals below 60 years of age but not in men. However, men are significantly protected from liver fibrosis by leisure-time PA [
103]. Therefore, promoting PA is crucial in preventing (and possibly reversing) liver fibrosis, and gender-specific strategies to achieve this goal need further exploration.
3.5. Cultural Attainment
In certain societies and cultures, gender can restrict access to education, which is a key indicator of socio-economic status [
104]. It is closely associated with the risk of developing psychological depression, MASLD, and metabolic syndrome (MetS) [
105,
106,
107]. Given these factors, advocating for equal opportunities in educational achievement should be a top priority for policymakers engaged in healthcare programs.
3.6. Health-Seeking Behavior
Women in Europe tend to take a more cautious approach to their health [
108], which may potentially enhance the protective effects of hormones against liver fibrosis. A study in Canada shows that women visit their primary care providers more frequently than men for both physical and mental health concerns. [
109]. Another study from India pinpoints gender differences in healthcare preferences, with women favoring socio-cultural and long-term approaches, while men prefer more technological and rapid therapies. [
110]. However, a large study in the USA among 3237 respondents (representing 4.6 million adults with CLDs) reports that cost-related medication nonadherence, along with food insecurity (which may be relevant for liver fibrosis), is more prevalent among younger individuals, women, those with low income, and those with multimorbidity [
111].
Collectively, these studies support the notion that gender influences health-seeking behavior in ways that are shaped by societal roles. However, further exploration is needed to understand the specific impact of these gender differences on liver fibrosis.
3.7. Liver Fibrosis in Cis vs. Transgender People
A large study involving 64,615,316 adults reported that 42,471 (0.07%) identify as transgender. Compared to cis gender adults, those who identify as transgender exhibit a two-fold increased prevalence of cirrhosis, often associated with anxiety, depression, or both [
112]. Gender-affirming hormone therapy (GAHT) is commonly administered to transgender individuals to alleviate dysphoria and improve quality of life. A large cohort including 1290 participants shows that estradiol administration in both cisgender and transgender individuals reduces the odds of MetS, while testosterone administration increases this risk. This is especially relevant for the management of MetS, cardiometabolic risk, and MASLD [
113], particularly among transgender individuals assigned male at birth, who seem to remain at higher risk of insulin resistance following GAHT [
114]. The risk of hepatobiliary cancers in those exposed to GAHT remains uncertain [
115], and GAHT poses challenges in the pre- and postoperative care of liver transplant patients [
116]. Therefore, further investigation into these obscure aspects of GAHT is warranted.
3.8. Does Physicians’ Sex Affect Liver Fibrosis Patients’ Outcome?
A groundbreaking study of 458,108 female and 318,819 male patients treated by either male or female physicians revealed that patients treated by female physicians experience lower rates of mortality and hospital readmission. The benefits of being treated by female physicians are even greater for female patients than male patients [
116]. This study provides strong evidence of an interaction between physicians’ and patients’ gender. The specific implications of this interaction in the hepatological arena, particularly for liver fibrosis patients, deserve further investigation.
4. Sex Differences in Liver-Related Outcomes
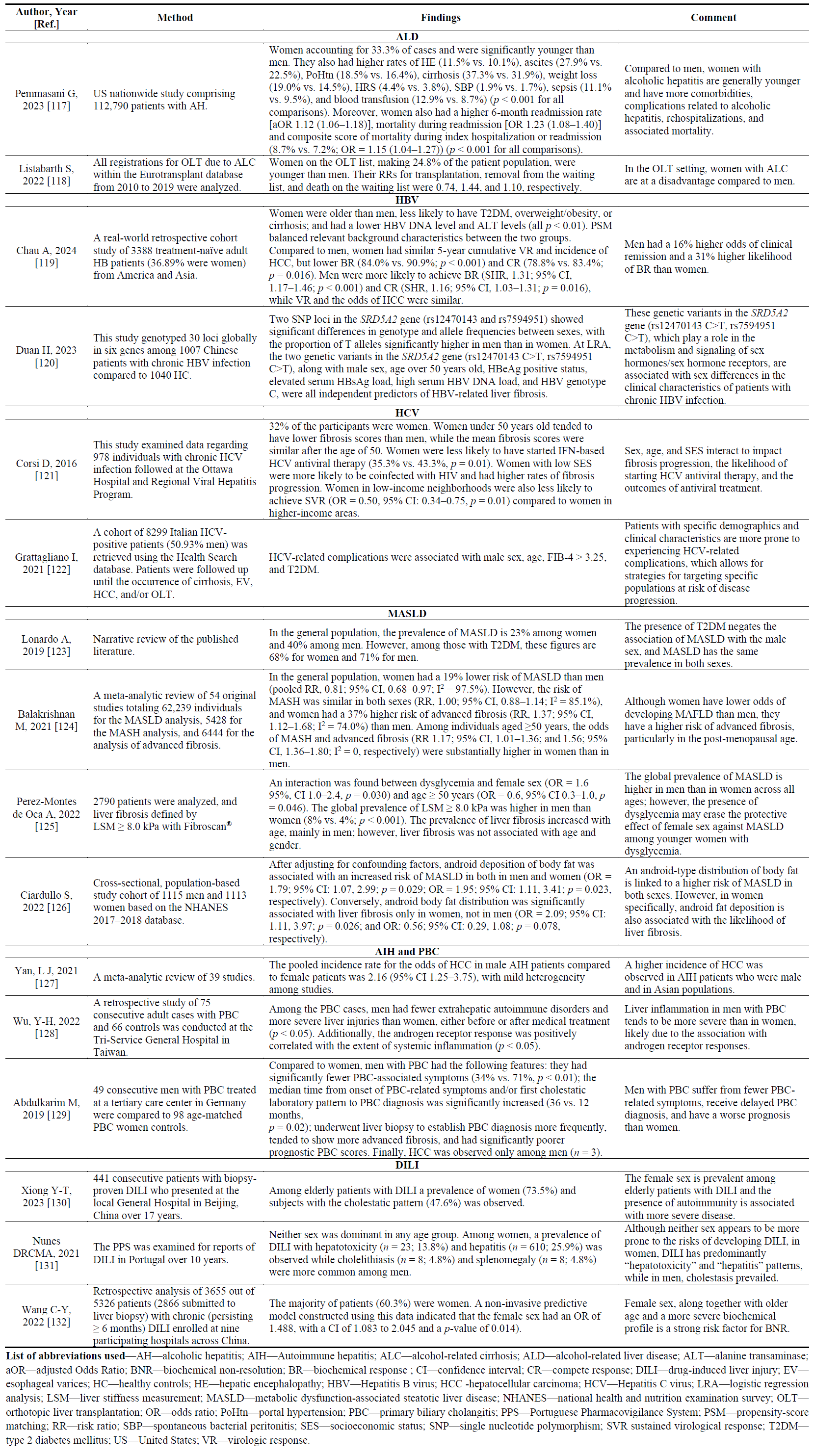
A robust body of published evidence supports the notion that certain liver-related complications show significant sex differences. These differences appear to depend on the etiology of liver disease, age, socio-economic status, and variable response rates to different treatment modalities. To summarize the topic, various etiologies are addressed, from alcohol to drug-induced liver injury (DILI) (). Studies were retrieved using the following research strategy (PubMed, accessed on 4 July 2024): (sex differences [Title/Abstract]) AND (liver fibrosis [Title/Abstract]).
. Sex differences across various etiologies of liver disease.
Alcohol-associated liver disease (ALD) accounts for nearly 5.1% of diseases and injuries worldwide and is one of the leading causes of death, directly linked to the amount of alcohol consumed [
133]. Alcohol use disorder (AUD), associated with heavy drinking, affects men more than women and is the second most disabling condition among men [
134]. AUD induces a wide spectrum of histological liver lesions, spanning from steatosis, hepatitis, fibrosis/cirrhosis, and HCC. Steatosis, the earliest form of liver injury, occurs in over 90% of heavy drinkers due to enhanced lipogenesis, increased fatty acid influx from adipose tissue, impaired LDL secretion, altered production of adipokines, reduced lipophagy, and diminished fatty acid oxidation [
135]. In some cases, steatosis progresses to steatohepatitis, which can lead to pericellular fibrosis and, eventually cirrhosis.
About one-third of heavy drinkers develop advanced liver disease, influenced by factors that may prevent, slow, or worsen disease progression [
135]. Men are more prone to alcohol consumption (68% vs. 64%) and AUD (7% vs. 4%) [
81]. However, women face a higher risk of ALD for the same alcohol intake levels [
136]. Several pathomechanisms may contribute to the increased prevalence and severity of ALD in women, including differences in hormone regulation of liver metabolism, estrogen-induced liver cell damage, inflammation, activation of Kupffer cells, and sustained liver injury progression. Other factors include variable estrogen receptor expression, differences in liver cell regeneration, alcohol-induced endotoxemia, and the differentially modulated activation of hepatoprotective genes in females. Women also experience more significant alcohol-induced changes in gut permeability [
137].
A recent experimental study using wild-type and protein arginine methyltransferase 6 (
Prmt6) knockout female mice subjected to either ovariectomy (OVX) or sham surgery and then fed a Western diet and alcohol shows that estrogen signaling suppresses the integrin pathway. This leads to a reduction in the expression of proinflammatory genes (Tnf, Il6) and profibrotic genes (Tgfb1, Col1a1), independent of PRMT6 levels [
39].
Women develop alcoholic hepatitis (AH) and alcohol-related cirrhosis (ALC) at a younger age than men. They also experience more complications, higher rehospitalization rates, and higher mortality [
117]. Additionally, women have less favorable outcomes in liver transplantation (LT) [
118]. Sex differences in the pathobiology of HCC have been extensively addressed elsewhere [
138]. Future studies should explore the pathogenic role of lipidomics, multi-omics, and other cutting-edge approaches in the development of progressive ALD [
139,
140].
4.2. Hepatitis B Virus
Although a vaccine against the Hepatitis B Virus (HBV) has been available for a long time, one-third of the world’s population has been infected with HBV. Nearly 1.5 million new individuals are infected yearly, and nearly 300 million people globally have chronic HBV infection [
141]. Sex disparity in HBV infection is well documented in both clinical setting and experimental studies [
142]. The men-to-women ratio increases with disease severity, ranging from 1.2 in asymptomatic carriers to 6.3 in chronic hepatitis B and 9.8 in hepatocellular carcinoma (HCC) [
143]. Among those vaccinated at birth and followed for over 18 years, 10.7% of men vs 4.4% of women are chronic carriers of HBV [
144]. Men with chronic hepatitis B tend to have higher HBV titer than women, even after adjusting for confounders [
145]. These findings suggest that sex disparities in HBV-induced HCC begin as early as the chronic hepatitis B stage, influenced by differences in HBV titers, immune response, or viral gene expression [
142].
Androgen and estrogen regulate the HBV life cycle differently by affecting viral transcription, HBV replication, and protein expression [
142]. Sex hormones also impact disease progression through HBV-specific immune responses [
142]. A recent study shows that men are 16% more likely than women to achieve clinical remission and 31% more likely to have a biochemical response [
119]. Two variants in the steroid 5-α-reductase type 2 (
SRD5A2) gene, involved in sex hormone metabolism and signaling, are associated with liver fibrosis in chronic hepatitis B [
120].
4.3. Hepatitis C Virus
Regardless of demographics and risk behaviors, women who inject drugs appear to be at a higher risk than men for acquiring HCV due to hormonal factors, social networks, and unequal access to healthcare [
146]. However, the female sex positively influences the progression and outcomes of chronic HCV infection. A study from 1978 on individuals with chronic hepatitis C shows that, compared to men, women have lower liver enzymes, lower HCV viral loads, lower weight, and are more likely to be infected with non-genotype-1 HCV. They are also more likely to be Black, Asian, or immigrants from Africa and Asia [
121]. Interestingly, pre-menopausal women have lower fibrosis scores than men. However, after the age of 50, the mean fibrosis scores become similar, suggesting a ‘catch-up’ phase [
121]. Moreover, low socioeconomic status (SES) is linked to a higher risk of HIV coinfection and faster fibrosis progression in women. Women from low-income areas are also less likely to achieve sustained virological response compared to those in higher-income regions [
121]. Collectively, these findings support the notion that sex and social factors influence fibrosis progression, likelihood of initiating HCV antiviral therapy, and treatment outcomes.
A recent study has identified significant sex differences and adverse events among individuals undergoing treatment for chronic hepatitis C or HIV/HCV co-infection with direct-acting antivirals (DAAs) [
147]. The data indicates that women with HCV genotype (GT) 1 or GT 3 infection have a significantly higher chance of achieving sustained virologic response (SVR) at 12-week post-treatment (SVR12) compared to men. These improved treatment outcomes in women compared to men are particularly noticeable among Whites, individuals aged 40 or older with GT1 or GT3 infections, and those aged 50 years and older, non-cirrhotic, and individuals with HCV GT3 infection who were treatment-experienced. However, these differences are not clinically relevant due to the high SVR12 rate achieved by both sexes. Women also experience milder side effects, but discontinuation rates are similar between men and women [
147]. Furthermore, a large study conducted on 15,295 subjects (40% women) found that SVR reduces the risk of extrahepatic complications such as acute coronary syndrome, end-stage renal disease, and ischemic stroke. This reduction is particularly significant in women, who should, therefore, be prioritized for DAAs treatment [
148]. Additionally, the male sex interacts with FIB-4 and diabetes in contributing to severe outcomes of fibrosis, such as cirrhosis, EV, HCC and/or OLT [
122]. Similar to HBV infection, in the case of HCV infection, sex hormones likely work together with the immune response to influence sex-dependent clinical outcomes [
149].
4.4. MASLD
The epidemiological features of sex differences in the MASLD arena have been extensively addressed elsewhere [
150,
151] and will not be reiterated here. In short, younger women are at a lower risk of MASLD than men, and this protection decreases after menopause [
57,
123]. However, this protection is rescinded by diabetes and dysglycemia [
125,
152]. Additionally, once MASLD is established, women are at a higher risk of advanced fibrosis than men, especially after the age of 50 [
124]. An android-type body fat deposition is associated with an increased risk of fibrosis in women regardless of body mass index (BMI) [
126]. Recent studies illustrate the synergistic interaction between genetics, sex hormones, and sex hormone receptors in the development of MASLD [
153,
154]. Sexual dimorphism of the innate immune system plays a significant (though under-appreciated) role in the pathogenesis of MASLD [
155]. Finally, sex hormones affect the severity of MASH via the pro-inflammatory TLR-MyD88-IL-6 signaling pathway [
156].
4.5. Autoimmune Hepatitis
Autoimmune hepatitis (AIH) is a chronic form of hepatitis strongly linked to genes that encode the HLA class II DRB1 alleles. It often develops after exposure to external triggers that cause molecular mimicry, leading to autoimmune responses that are worsened by impaired T-cell regulation [
157]. Women generally have a higher risk of developing AIH compared to men [
75,
158]. However, men face an increased risk of developing HCC in cases of AIH [
127]. This risk is connected to the progression of hepatic fibrosis, which involves various factors contributing to fibrosis, such as inflammation, cell apoptosis, and oxidative stress [
157]. The chronic inflammation in the liver is mainly driven by autoimmune processes that attract monocytes and macrophages, activating Toll-like receptors (TLRs) in HSCs and Kupffer cells. Cytokines and chemokines then enhance the response of HSCs through factors like transforming growth factor-β (TGF-β), the proinflammatory tumor necrosis factor-α (TNF-α), interleukin-1β (IL-1β), and chemokine ligands [
157].
The generation of apoptotic bodies is the second main mechanism involved in fibrotic progression in AIH [
157]. Finally, increased oxidative stress, facilitated by impaired antioxidant status in these individuals, also contributes to the fibrogenic process in AIH [
159]. Sex hormones, which regulate each of the above pathogenic steps [
62,
160], position themselves as the ideal target for innovative treatment.
4.6. Primary Biliary Cholangitis
Primary biliary cholangitis (PBC) is a chronic cholestatic disease characterized by the non-suppurative destruction of small and medium bile ducts, ultimately leading to fibrosis and cirrhosis in some individuals. PBC is more commonly diagnosed in women, especially during and after menopause, with a female-to-male ratio of approximately 4:1 [
161]. However, in men, PBC is often diagnosed later, progresses more rapidly, and is linked to a poorer prognosis and higher all-cause mortality [
128,
129]. Nevertheless, experts believe sex differences in PBC are gradually becoming less pronounced [
162,
163]. The interaction between cholangiocytes and sex hormones in the cholestasis associated with PBC has been extensively reviewed in other studies [
161].
4.7. Primary Sclerosing Cholangitis
Primary sclerosing cholangitis (PSC) is a chronic cholestatic autoimmune condition characterized by inflammation, fibrosis, and stricturing of intrahepatic and/or extrahepatic biliary ducts [
164]. PSC tends to affect men more often (up to 60%) than women, with the average age at diagnosis being around 40 years [
161]. The prevalence rate of PSC is reportedly increasing globally due to the widespread use of magnetic resonance cholangiopancreatography and endoscopic retrograde cholangiopancreatography. Although PBC and PSC are cholestatic disorders, the reasons for their markedly contrasting sex distribution are not fully understood. One possible explanation involves the enzyme cytochrome P450 3A4, which is up-regulated by the farnesoid X receptor (FXR) to protect against cholestasis. This enzyme is more elevated in premenopausal women than men, but its effectiveness decreases in the presence of high bile acid levels and significantly decreases after menopause [
161]. The association of PSC with ulcerative colitis may offer further insights into the role of the gut microbiome in the pathogenesis of cholestasis [
164].
4.8. Drug-Induced Liver Injury
The prevalence of drug-induced liver injury (DILI) is higher among elderly women [
130], and women also exhibit more severe inflammatory liver histology [
131]. Being female is a significant risk factor for the failure of chronic DILI to resolve biochemically [
132].
Next, we will discuss specific liver-related complications ranging from portal hypertension to HCC (). The studies were identified using the same research methodology outlined previously.
. Relation of sex with individual complications of liver fibrosis.
Variceal bleeding, as opposed to non-variceal bleeding, is linked to higher mortality rates in men but not in women [
165]. If these results are confirmed by larger studies, they could potentially support sex-specific clinical management approaches depending on the type of bleeding identified through endoscopy.
4.10. Hepatic Encephalopathy
Compared to men, women are at a significantly higher risk of hepatic encephalopathy (HE) [
166]. The different compositions of intestinal microbiota may account for this disparity and the sex differences in responses to HE therapies [
48].
4.11. Hepatocellular Carcinoma
Sex hormones can have either a protective or harmful effect on both sexes, influenced by factors such as BMI, alcohol consumption, active smoking, and social determinants [
138]. Sexual dimorphism is a common feature of HCC, with men at the highest risk, especially in virus-related chronic liver disease (CLD) [
171,
172]. Male sex, diabetes, and liver fibrosis predict the risk of HCC after DAAs therapy [
167]. However, female sex is not an independent predictor of survival [
168], while MAFLD is a significant risk factor for mortality in women [
169]. Women who undergo liver resection have a lower risk of post-hepatectomy liver failure [
170], likely due to sex hormone-related differences in hepatic regeneration [
173].
In conclusion, significant sex differences characterize the epidemiological and clinical features of various types of CLD and the specific complications of liver fibrosis. Collectively, these sex differences may potentially influence clinical outcomes and provide a basis for sex-specific precision medicine approaches.
5. Sex Differences in Extra-Hepatic Outcomes
The spectrum of health issues associated with liver fibrosis in the context of MASLD is broad. It has recently expanded to include extra-hepatic cancers such as gynecological cancers and malignant neoplasms of the gastro-intestinal tract. These have been extensively discussed in recent literature [
174,
175] and will not be reiterated here. Therefore, among the various extra-hepatic outcomes associated with advanced liver fibrosis, we will focus on sarcopenia, CVD, diabetes, CKD, and dementia. These conditions have the potential to impact quality of life and life expectancy.
5.1. Sarcopenia
Defined as the “
progressive and generalized loss of muscle mass and strength”, sarcopenia is a common feature of liver cirrhosis that negatively affects patient outcomes while on a liver transplantation (LT) waiting list, as well as after LT and during HCC treatment [
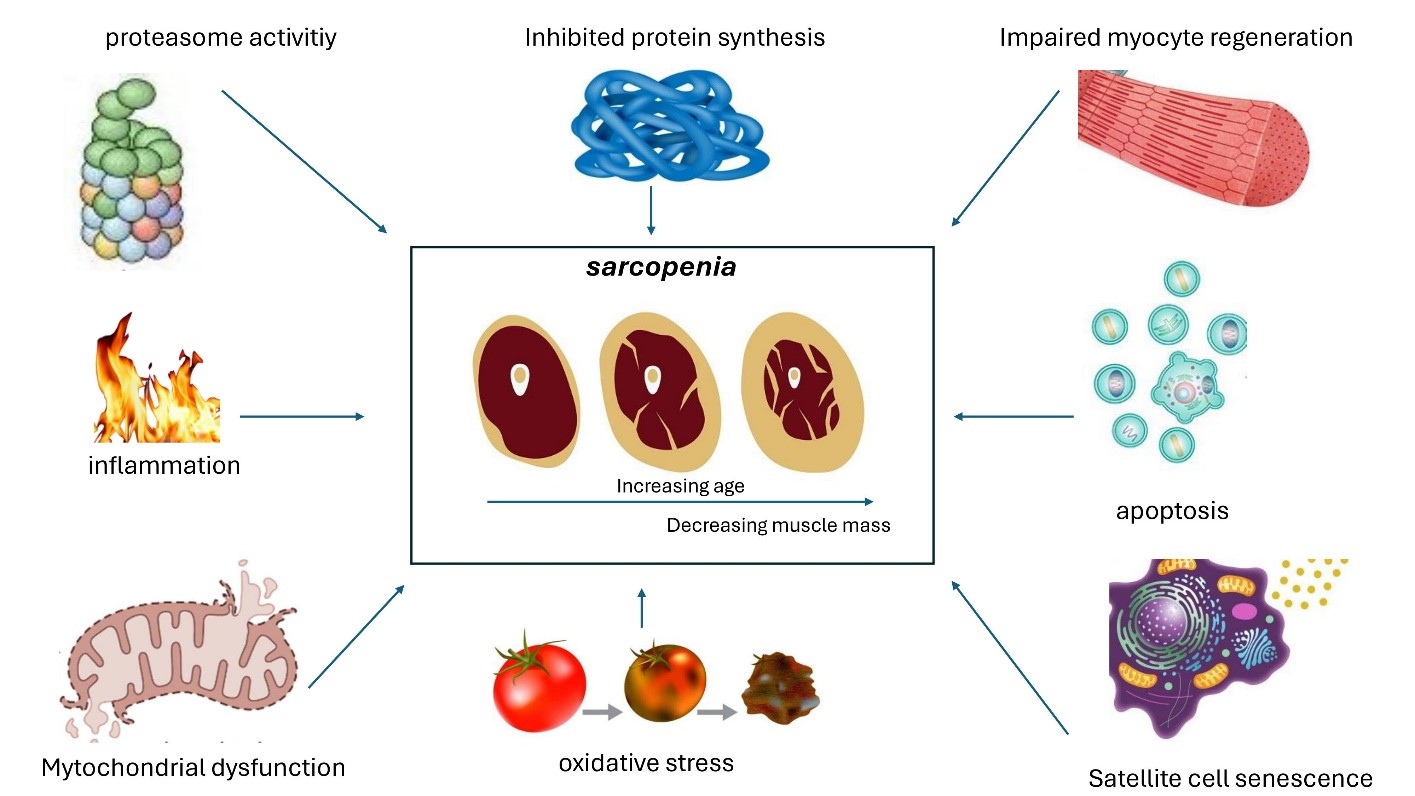
176]. Various pathomechanisms may be responsible for the development of sarcopenia in patients with cirrhosis ().
. Pathogenesis of sarcopenia associated with advanced liver fibrosis. Schematic illustration of the multiple cellular and molecular mechanisms involved in the development of sarcopenia [
177].
Furthermore, a proof-of-concept cross-sectional study demonstrates that individuals with liver cirrhosis and muscle wasting have an altered gut microbiome composition [
178]. A recent meta-analytic review of 63,330 patients and 29 studies finds a strong association of sarcopenia with MASLD (aOR 2.08, 95% CI 1.58–2.74, I
2 = 93.6%) irrespective of stratification by confounding factors [
179]. Moreover, this study also shows an association of sarcopenia with poor prognosis in MASLD (aHR 1.59, 95% CI 1.33–1.91, I
2 = 0%) [
179]. Most published investigations concur that men exhibit a higher prevalence of sarcopenia, possibly owing to anatomy-related causes [
176,
180]. However, the retrospective study design and different diagnostic criteria for sarcopenia hinder our understanding of sex differences in this area [
176,
180].
5.2. Cardiovascular Disease
The stage of liver fibrosis is a principal risk modifier of CVD among individuals with fibrosing MASLD. Vilar-Gomez, Calzadilla Bertot and their colleagues conducted a collaborative study involving 458 patients with biopsy-proven MASLD. Among these patients, 159 had bridging fibrosis (F3) and 222 had class A Child-Turcotte-Pugh compensated cirrhosis. The study took place from 1995 to 2013 and follow-up continued until December 2016 [
8]. The authors found that individuals with MASLD-cirrhosis primarily experienced liver-related events, while those with bridging fibrosis were more prone to extra-hepatic cancers and vascular events [
8].
Recent evidence suggests that regardless of the diagnostic terminology used (NAFLD or MAFLD), the risk of developing CVD events is not significantly different between the two definitions. However, MAFLD is associated with a higher number of CVD events compared to NAFLD [
181]. It is important to note that MASLD is strongly linked to an increased risk of CVD events, with this risk further escalating in the presence of advanced stages of liver fibrosis [
182]. In the realm of gender-specific medicine, alcohol consumption, which is more commonly associated with males, particularly in the context of MetALD, a subtype of SLD, is linked to the highest odds of CVD [
81]. This was revealed in a Korean Genome and Epidemiology study involving 9497 participants followed for 17.5 years [
183]. On the other hand, cryptogenic SLD, representing 3.5% of SLD patients, carries the lowest risk of CVD [
184].
Sex also plays a key role in CVD risk in the MASLD arena, as reported by Ren et al. [
185]. These authors analyzed data from adults in the National Health and Nutrition Examination Surveys from 2000–2014 and found that men have a significantly higher all-cause mortality rate compared to women (12.4% vs. 7.7%;
p = 0.005). The risk of CVD death is higher in women aged 60 or younger with NAFLD (adjusted hazard ratio [aHR]: 0.214, 95% CI: 0.053–0.869,
p = 0.031). Men with a BMI > 30 kg/m
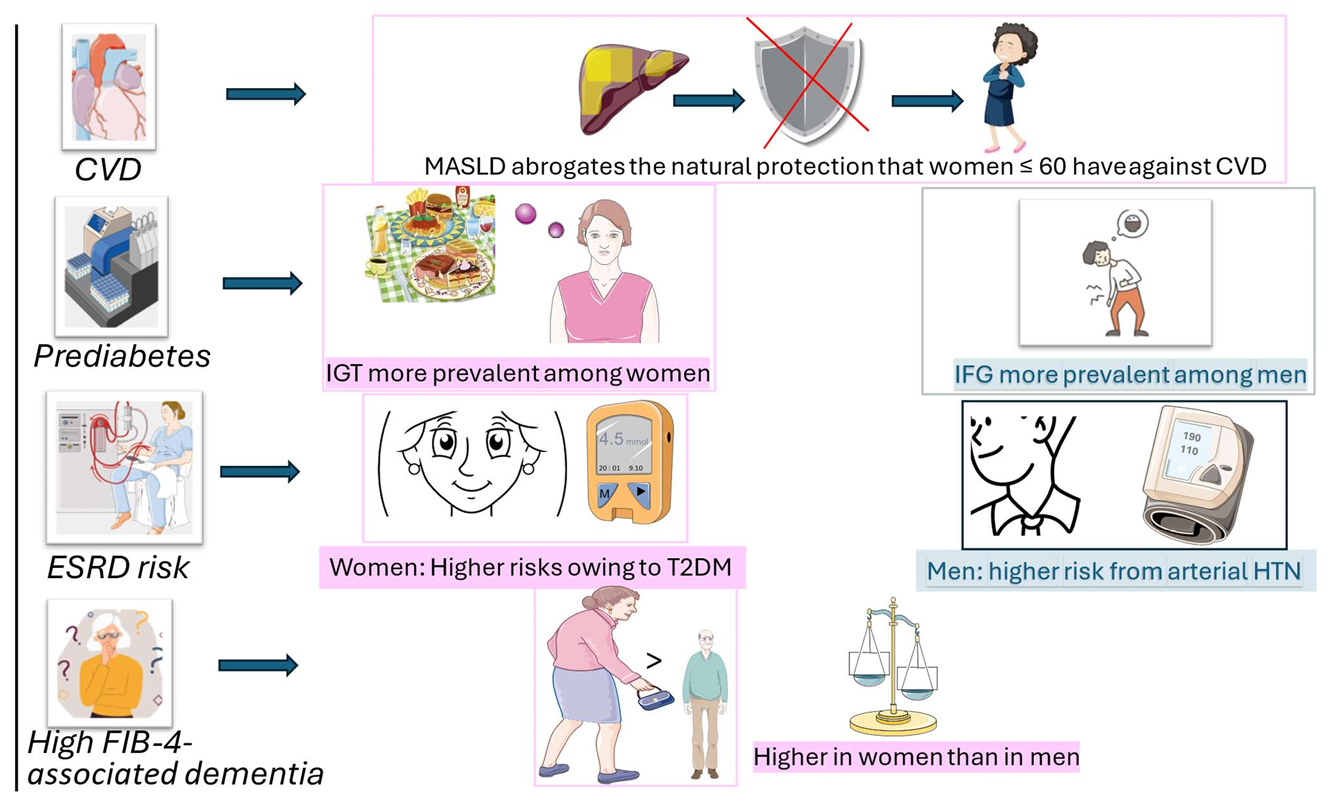
2 and diabetes show a higher risk of all-cause mortality. However, sex differences in CVD events are not as apparent in patients aged over 60 years. Despite some methodological limitations, the study by Ren et al. suggests that MASLD eliminates the natural protection women have from CVD, which is in line with previous studies [
186].
Another example of sexual dimorphism in the association between liver fibrosis and major events of CVD comes from the study by Parikh et al. [
187]. These authors studied 572 participants with incident ischemic stroke and 1104 participants in a stratified cohort random sample, following them for ischemic stroke. They found that advanced liver fibrosis, as assessed by FIB-4 and NFS, is linked to a higher risk of ischemic stroke in women but not in men.
5.3. Diabetes and Impaired Glucose Tolerance
Sex-specific differences exist in the categories of prediabetes. Impaired glucose tolerance, which reflects postprandial insulin resistance, is more prevalent in women than in men. On the other hand, impaired fasting blood glucose, which reflects fasting insulin resistance, is more prevalent in men than in women [
75]. Additionally, the risk of developing impaired glucose tolerance (IGT) is influenced by pregnancy and menopause [
188]. A strong, likely bidirectional relationship exists between liver fibrosis and type 2 diabetes mellitus (T2DM) across various forms of CLD, with the most well-characterized being SLD resulting from chronic HCV infection and NAFLD/MASLD [
189,
190]. Mantovani et al., in a meta-analysis of 33 studies including 501,022 individuals, show that over a median follow-up of 5 years, NAFLD is associated with a higher risk of developing diabetes compared to NAFLD-free controls (
n = 26 studies; random-effects HR 2.19, 95% CI 1.93–2.48; I
2 = 91.2%). Interestingly, subjects with more ‘severe’ NAFLD face higher odds of incident diabetes (
n = 9 studies; random-effects HR 2.69, 95% CI 2.08 to 3.49; I
2 = 69%), and this risk markedly increases with the severity of liver fibrosis (
n = 5 studies; random-effects HR 3.42, 95% CI 2.29 to 5.11; I
2 = 44.6%), regardless of common metabolic confounding risk factors [
191]. Additional investigation is warranted to address the various genetic, hormonal, and lifestyle factors that differently modulate the odds of IGT and T2DM among men and women with fibrosing CLD.
5.4. Chronic Kidney Disease
A robust body of published literature supports that MASLD is a risk factor for incident and prevalent CKD assessed with either estimated glomerular filtration rate (eGFR) < 60 mL/h or proteinuria [
192,
193,
194,
195]. While some studies show no association [
196], other researchers suggest that steatosis, rather than liver fibrosis, maybe the key driver of CKD risk in MASLD [
197]. This could be due to the fact that steatosis, in turn, is the precursor of fibrosis in MASLD via steatohepatitis [
198]. Sexual medicine approaches in the realm of CKD associated with MASLD are not yet fully developed, and information seems scarce and preliminary. A meta-analysis published in 2017 [
199] found no significant difference between the sexes in diabetes-related CKD, with a pooled adjusted women-to-men relative risk ratio of 1.14 (95% CI 0.97, 1.34). However, among individuals with diabetes, women have a higher risk of end-stage renal disease (ESRD) than men, indicating a greater risk of CKD progression among women. This could be linked to autoimmune mechanisms to which women are more susceptible than men [
200]. Conversely, men seem to have a higher risk of CKD and ESRD compared to women, primarily driven by arterial hypertension, as supported by strong meta-analytic evidence [
201]. This difference may be influenced by sex hormones affecting vascular tone, oxidative stress, inflammation, and apoptosis [
202], as well as variations in the function of endothelin receptors (ET-B vs. ET-A) between the sexes [
203].
Hyperuricemia is also identified as a potential risk factor for liver fibrosis in MASLD [
204,
205,
206], although findings are conflicting [
207]. Interestingly, the female sex may be protected from some of the harmful outcomes of hyperuricemia, including renal disease, CVD, and metabolic syndrome [
208]. Finally, a study conducted in a cohort of 432 patients with CLD of varying etiologies found that the female sex, together with CKD, was associated with muscle cramps in CLD [
209], supporting further investigation into this association.
5.5. Dementia
Research on the impact of MASLD on cognitive function, particularly dementia, yields conflicting results [
210,
211,
212,
213,
214,
215]. A meta-analysis of seven prospective cohorts reports that MASLD does not significantly increase the risk of dementia (HR: 1.01). However, other studies demonstrate that the presence of liver fibrosis in MASLD patients markedly elevates this risk [
19,
211,
216,
217]. For instance, a nationwide retrospective cohort study by Weinstein et al. [
218] finds that over a median follow-up of 17 years, individuals with a FIB-4 > 2.67 have an 18% increased risk of developing dementia. Similarly, a study by Parikh et al. [
219], using data from the UK Biobank, reports a 52% increased risk of dementia associated with FIB-4 > 2.67 over a median follow-up of 9 years. However, these studies differ in both the magnitude of dementia risk associated with liver fibrosis and the role of sex differences in this relationship. These discrepancies are likely due to variations in methods and sample selection, including differences in follow-up duration and the prevalence of fibrosis in the study populations. While Parikh et al. [
219] found no significant modification of dementia risk by sex, Weinstein et al. [
218] demonstrated that the risk of dementia associated with advanced fibrosis (FIB-4 > 2.67) was higher in females than in males (22% vs. 17%). The more pronounced sex differences observed with longer follow-up (17 years vs. 9 years) suggest that the moderating role of liver fibrosis in the relationship between sex and dementia may increase with age, becoming more prominent in later life.
Several factors could explain this modifying effect. The progression to advanced fibrosis accelerates in females during later life [
124], particularly after menopause [
25]—a period when the majority of dementia cases occur. This accelerated fibrosis may exacerbate underlying pathophysiological processes that lead to cognitive decline, such as impaired clearance of peripheral amyloid-beta (Aβ) [
220], inflammation [
221,
222], gut dysbiosis [
223,
224,
225,
226], and vascular damage [
227,
228,
229,
230].
In summary, although data on the relationship between sex, liver fibrosis, and dementia are limited, preliminary studies suggest that sex differences may influence the impact of liver fibrosis on the risk of dementia. summarizes the principal notions discussed in Section 5.
. Overview of extrahepatic outcomes in MASLD. Legend to . This cartoon, based on the bibliographic references discussed in the text, specifically focuses on sex differences in cardio-nephro-metabolic risk. Moreover, sex differences in dementia associated with liver fibrosis are highlighted. CVD—cardiovascular disease; ESRD—end-stage renal disease; FIB-4—fibrosis 4; HTN—hypertension; IFG—impaired fasting glucose; IGT—impaired glucose tolerance; MASLD—metabolic dysfunction-associated steatotic liver disease; T2DM—type 2 diabetes mellitus.
6. Conclusions
Sex and gender differences play a significant role in the profibrogenic pathomechanisms that impact the prevalence, severity, and outcomes of liver fibrosis. Genetic factors, hormonal influences, immune responses, and lifestyle choices contribute to these disparities between men and women. Generally, females have a lower risk of fibrosis due to protective genetic and hormonal factors, such as estrogen’s anti-fibrogenic properties and a more balanced immune response. Conversely, males are more prone to fibrosis due to factors like testosterone’s fibrogenic effects, higher levels of pro-inflammatory cytokines, and riskier lifestyle behaviors. Additionally, sex differences in the gut microbiota further modulate the progression of liver fibrosis, with males showing a tendency for more severe fibrosis linked to inflammation-inducing gut bacteria. The exploration of sex differences in liver-related outcomes also reveals substantial disparities that vary depending on the etiology of liver disease, age, and other factors such as socio-economic status and treatment responses. Women have distinct vulnerabilities and outcomes compared to men across various liver diseases, from alcohol-related liver disease to MASLD, AIH, and DILI. Similarly, sex differences significantly impact the risk and progression of extra-hepatic outcomes, including sarcopenia, CVD, diabetes, CKD, and dementia.
Collectively, the evidence underscores the necessity of a sex-specific approach in the management of CLD and its complications. Such an approach could potentially optimize outcomes by addressing the unique risk profiles and therapeutic needs of men and women, while also revealing novel therapeutic targets. Further research is warranted to deepen our understanding of these sex-specific mechanisms and to translate this knowledge into precision medicine strategies that improve patient care and prognosis for both genders.
Acknowledgments
Attribution for the icons used in Figure 2 and Figure 3, and graphical abstract: Icons created by Freepik from www.flaticon.com (accessed on 27 September 2024). Figure 5 was created using SMART (Servier Medical Art) from https://smart.servier.com/ (accessed on 27 September 2024).
Author Contributions
All authors contributed equally to Conceptualization, Methodology, Data Curation, Writing, Review & Editing of this manuscript.
Ethics Statement
Not applicable.
Informed Consent Statement
Not applicable.
Funding
This research received no external funding.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence this paper.
References
1.
Bataller R, Brenner DA. Liver fibrosis.
J. Clin. Investig. 2005,
115, 209–218.
[Google Scholar]
2.
Taylor RS, Taylor RJ, Bayliss S, Hagström H, Nasr P, Schattenberg JM, et al. Association Between Fibrosis Stage and Outcomes of Patients With Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis.
Gastroenterology 2020,
158, 1611–1625.e12.
[Google Scholar]
3.
Kuchay MS, Martínez-Montoro JI, Kaur P, Fernández-García JC, Ramos-Molina B. Non-alcoholic fatty liver disease-related fibrosis and sarcopenia: An altered liver-muscle crosstalk leading to increased mortality risk.
Ageing Res. Rev. 2022,
80, 101696.
[Google Scholar]
4.
Petta S, Ciminnisi S, Di Marco V, Cabibi D, Cammà C, Licata A, et al. Sarcopenia is associated with severe liver fibrosis in patients with non-alcoholic fatty liver disease.
Aliment. Pharmacol. Ther. 2017,
45, 510–518.
[Google Scholar]
5.
Lee YH, Kim SU, Song K, Park JY, Kim DY, Ahn SH, et al. Sarcopenia is associated with significant liver fibrosis independently of obesity and insulin resistance in nonalcoholic fatty liver disease: Nationwide surveys (KNHANES 2008–2011).
Hepatology 2016,
63, 776–786.
[Google Scholar]
6.
Wijarnpreecha K, Kim D, Raymond P, Scribani M, Ahmed A. Associations between sarcopenia and nonalcoholic fatty liver disease and advanced fibrosis in the USA.
Eur. J. Gastroenterol. Hepatol. 2019,
31, 1121–1128.
[Google Scholar]
7.
Henson JB, Simon TG, Kaplan A, Osganian S, Masia R, Corey KE. Advanced fibrosis is associated with incident cardiovascular disease in patients with non-alcoholic fatty liver disease.
Aliment. Pharmacol. Ther. 2020,
51, 728–736.
[Google Scholar]
8.
Vilar-Gomez E, Calzadilla-Bertot L, Wai-Sun Wong V, Castellanos M, Aller-de la Fuente R, Metwally M, et al. Fibrosis Severity as a Determinant of Cause-Specific Mortality in Patients With Advanced Nonalcoholic Fatty Liver Disease: A Multi-National Cohort Study.
Gastroenterology 2018,
155, 443–457.e17.
[Google Scholar]
9.
Cardoso CRL, Villela-Nogueira CA, Leite NC, Salles GF. Prognostic impact of liver fibrosis and steatosis by transient elastography for cardiovascular and mortality outcomes in individuals with nonalcoholic fatty liver disease and type 2 diabetes: The Rio de Janeiro Cohort Study.
Cardiovasc. Diabetol. 2021,
20, 193.
[Google Scholar]
10.
Shili-Masmoudi S, Wong GL, Hiriart JB, Liu K, Chermak F, Shu SS, et al. Liver stiffness measurement predicts long-term survival and complications in non-alcoholic fatty liver disease.
Liver Int. 2020,
40, 581–589.
[Google Scholar]
11.
Anstee QM, Berentzen TL, Nitze LM, Jara M, Jensen AB, Kjær MS, et al. Prognostic utility of Fibrosis-4 Index for risk of subsequent liver and cardiovascular events, and all-cause mortality in individuals with obesity and/or type 2 diabetes: A longitudinal cohort study.
Lancet Reg. Health Eur. 2024,
36, 100780.
[Google Scholar]
12.
Baratta F, Pastori D, Angelico F, Balla A, Paganini AM, Cocomello N, et al. Nonalcoholic Fatty Liver Disease and Fibrosis Associated With Increased Risk of Cardiovascular Events in a Prospective Study.
Clin. Gastroenterol. Hepatol. 2020,
18, 2324–2331.e4.
[Google Scholar]
13.
Tamaki N, Higuchi M, Kurosaki M, Loomba R, Izumi N. Risk Difference of Liver-Related and Cardiovascular Events by Liver Fibrosis Status in Nonalcoholic Fatty Liver Disease.
Clin. Gastroenterol. Hepatol. 2022,
20, 1171–1173.e2.
[Google Scholar]
14.
Ekstedt M, Hagström H, Nasr P, Fredrikson M, Stål P, Kechagias S, et al. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up.
Hepatology 2015,
61, 1547–1554.
[Google Scholar]
15.
Seo DH, Suh YJ, Cho Y, Ahn SH, Seo S, Hong S, et al. Advanced Liver Fibrosis Is Associated with Chronic Kidney Disease in Patients with Type 2 Diabetes Mellitus and Nonalcoholic Fatty Liver Disease.
Diabetes Metab. J. 2022,
46, 630–639.
[Google Scholar]
16.
Sun Y, Hong L, Huang Z, Wang L, Xiong Y, Zong S, et al. Fibrosis Risk in Nonalcoholic Fatty Liver Disease Is Related to Chronic Kidney Disease in Older Type 2 Diabetes Patients.
J. Clin. Endocrinol. Metab. 2022,
107, e3661–e3669.
[Google Scholar]
17.
Zuo G, Xuan L, Xin Z, Xu Y, Lu J, Chen Y, et al. New Nonalcoholic Fatty Liver Disease and Fibrosis Progression Associate With the Risk of Incident Chronic Kidney Disease.
J. Clin. Endocrinol. Metab. 2021,
106, e3957–e3968.
[Google Scholar]
18.
Moh MC, Pek SLT, Sze KCP, Low S, Subramaniam T, Ang K, et al. Associations of non-invasive indices of liver steatosis and fibrosis with progressive kidney impairment in adults with type 2 diabetes.
Acta Diabetol. 2023,
60, 827–835.
[Google Scholar]
19.
Weinstein G, Davis-Plourde K, Himali JJ, Zelber-Sagi S, Beiser AS, Seshadri S. Non-alcoholic fatty liver disease, liver fibrosis score and cognitive function in middle-aged adults: The Framingham Study.
Liver Int. 2019,
39, 1713–1721.
[Google Scholar]
20.
Zamani M, Alizadeh-Tabari S, Ajmera V, Singh S, Murad MH, Loomba R. Global prevalence of advanced liver fibrosis and cirrhosis in the general population: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2024. doi:10.1016/j.cgh.2024.08.020.
21.
Cooper KM, Delk M, Devuni D, Sarkar M. Sex differences in chronic liver disease and benign liver lesions.
JHEP Rep. 2023,
5, 100870.
[Google Scholar]
22.
Caballería L, Pera G, Arteaga I, Rodríguez L, Alumà A, Morillas RM, et al. High Prevalence of Liver Fibrosis Among European Adults With Unknown Liver Disease: A Population-Based Study.
Clin. Gastroenterol. Hepatol. 2018,
16, 1138–1145.e5.
[Google Scholar]
23.
Ozdemir BH, Ozgun G, Akdur A, Moray G, Haberal M. Hepatic Estrogen Receptor Expression Prevents Liver Fibrosis through Decreasing the Risk of Early Activation of Hepatic Stellate Cells.
Transplantation 2018,
102, S385.
[Google Scholar]
24.
Zhang B, Zhang CG, Ji LH, Zhao G, Wu ZY. Estrogen receptor β selective agonist ameliorates liver cirrhosis in rats by inhibiting the activation and proliferation of hepatic stellate cells.
J. Gastroenterol. Hepatol. 2018,
33, 747–755.
[Google Scholar]
25.
Yang JD, Abdelmalek MF, Pang H, Guy CD, Smith AD, Diehl AM, et al. Gender and menopause impact severity of fibrosis among patients with nonalcoholic steatohepatitis.
Hepatology 2014,
59, 1406–1414.
[Google Scholar]
26.
Dunn SE, Perry WA, Klein SL. Mechanisms and consequences of sex differences in immune responses.
Nat. Rev. Nephrol. 2024,
20, 37–55.
[Google Scholar]
27.
Lovejoy JC, Champagne CM, de Jonge L, Xie H, Smith SR. Increased visceral fat and decreased energy expenditure during the menopausal transition.
Int. J. Obes. 2008,
32, 949–958.
[Google Scholar]
28.
Link JC, Reue K. Genetic Basis for Sex Differences in Obesity and Lipid Metabolism.
Annu. Rev. Nutr. 2017,
37, 225–245.
[Google Scholar]
29.
Abdel-Gawad M, Nour M, El-Raey F, Nagdy H, Almansoury Y, El-Kassas M. Gender differences in prevalence of hepatitis C virus infection in Egypt: A systematic review and meta-analysis.
Sci. Rep. 2023,
13, 2499.
[Google Scholar]
30.
Nagral A, Bangar M, Menezes S, Bhatia S, Butt N, Ghosh J, et al. Gender Differences in Nonalcoholic Fatty Liver Disease.
Euroasian J. Hepatogastroenterol. 2022,
12 (Suppl 1), S19–S25.
[Google Scholar]
31.
Wu XN, Wang MZ, Zhang N, Zhang W, Dong J, Ke MY, et al. Sex-determining region Y gene promotes liver fibrosis and accounts for sexual dimorphism in its pathophysiology.
J. Hepatol. 2024,
80, 928–940.
[Google Scholar]
32.
Xu JW, Gong J, Chang XM, Luo JY, Dong L, Jia A, et al. Effects of estradiol on liver estrogen receptor-alpha and its mRNA expression in hepatic fibrosis in rats.
World J. Gastroenterol. 2004,
10, 250–254.
[Google Scholar]
33.
Bernardi S, Toffoli B, Tonon F, Francica M, Campagnolo E, Ferretti T, et al. Sex Differences in Proatherogenic Cytokine Levels.
Int. J. Mol. Sci. 2020,
21, 3861.
[Google Scholar]
34.
Athwal VS, Pritchett J, Llewellyn J, Martin K, Camacho E, Raza SM, et al. SOX9 predicts progression toward cirrhosis in patients while its loss protects against liver fibrosis.
EMBO Mol. Med. 2017,
9, 1696–1710.
[Google Scholar]
35.
Horn P, Tacke F. Metabolic reprogramming in liver fibrosis.
Cell Metab. 2024,
36, 1439–1455.
[Google Scholar]
36.
Day CP. Genetic studies to identify hepatic fibrosis genes and SNPs in human populations.
Methods Mol. Med. 2005,
117, 315–331.
[Google Scholar]
37.
Balcar L, Semmler G, Oberkofler H, Zandanell S, Strasser M, Datz L, et al. PNPLA3 is the dominant SNP linked to liver disease severity at time of first referral to a tertiary center.
Dig. Liver Dis. 2022,
54, 84–90.
[Google Scholar]
38.
Wegermann K, Garrett ME, Zheng J, Coviello A, Moylan CA, Abdelmalek MF, et al. Sex and Menopause Modify the Effect of Single Nucleotide Polymorphism Genotypes on Fibrosis in NAFLD.
Hepatol. Commun. 2021,
5, 598–607.
[Google Scholar]
39.
Nataraj K, Schonfeld M, Rodriguez A, Tikhanovich I. Protective role of 17β-estradiol in alcohol-associated liver fibrosis is mediated by suppression of integrin signaling.
Hepatol. Commun. 2024,
8, e0428.
[Google Scholar]
40.
Milette S, Hashimoto M, Perrino S, Qi S, Chen M, Ham B, et al. Sexual dimorphism and the role of estrogen in the immune microenvironment of liver metastases.
Nat. Commun. 2019,
10, 5745.
[Google Scholar]
41.
Sarkar MA, Suzuki A, Abdelmalek MF, Yates KP, Wilson LA, Bass NM, et al. Testosterone is Associated With Nonalcoholic Steatohepatitis and Fibrosis in Premenopausal Women With NAFLD.
Clin. Gastroenterol. Hepatol. 2021,
19, 1267–1274.e1.
[Google Scholar]
42.
Xu L, Yuan Y, Che Z, Tan X, Wu B, Wang C, et al. The Hepatoprotective and Hepatotoxic Roles of Sex and Sex-Related Hormones.
Front. Immunol. 2022,
13, 939631.
[Google Scholar]
43.
Targher G, Bertolini L, Rodella S, Zoppini G, Zenari L, Falezza G. Associations between liver histology and cortisol secretion in subjects with nonalcoholic fatty liver disease.
Clin. Endocrinol. 2006,
64, 337–341.
[Google Scholar]
44.
Miyauchi S, Miyake T, Miyazaki M, Eguchi T, Niiya T, Yamamoto S, et al. Insulin-like growth factor-1 is inversely associated with liver fibrotic markers in patients with type 2 diabetes mellitus.
J. Diabetes Investig. 2019,
10, 1083–1091.
[Google Scholar]
45.
Wauthier V, Sugathan A, Meyer RD, Dombkowski AA, Waxman DJ. Intrinsic sex differences in the early growth hormone responsiveness of sex-specific genes in mouse liver.
Mol. Endocrinol. 2010,
24, 667–678.
[Google Scholar]
46.
Sayaf K, Zanotto I, Gabbia D, Alberti D, Pasqual G, Zaramella A, et al. Sex Drives Functional Changes in the Progression and Regression of Liver Fibrosis.
Int. J. Mol. Sci. 2023,
24, 16452.
[Google Scholar]
47.
Scotland RS, Stables MJ, Madalli S, Watson P, Gilroy DW. Sex differences in resident immune cell phenotype underlie more efficient acute inflammatory responses in female mice.
Blood 2011,
118, 5918–5927.
[Google Scholar]
48.
Saboo K, Shamsaddini A, Iyer MV, Hu C, Fagan A, Gavis EA, et al. Sex is associated with differences in gut microbial composition and function in hepatic encephalopathy.
J. Hepatol. 2021,
74, 80–88.
[Google Scholar]
49.
Shi J, Yang Y, Xu W, Cai H, Wu J, Long J, et al. Sex-Specific Associations between Gut Microbiome and Non-Alcoholic Fatty Liver Disease among Urban Chinese Adults.
Microorganisms 2021,
9, 2118.
[Google Scholar]
50.
Glass LM, Hunt CM, Fuchs M, Su GL. Comorbidities and Nonalcoholic Fatty Liver Disease: The Chicken, the Egg, or Both?
Fed. Pract. 2019,
36, 64–71.
[Google Scholar]
51.
Kezer CA, Simonetto DA, Shah VH. Sex Differences in Alcohol Consumption and Alcohol-Associated Liver Disease.
Mayo Clin. Proc. 2021,
96, 1006–1016.
[Google Scholar]
52.
Yabe Y, Kim T, Oh S, Shida T, Oshida N, Hasegawa N, et al. Relationships of Dietary Habits and Physical Activity Status with Non-Alcoholic Fatty Liver Disease Featuring Advanced Fibrosis.
Int. J. Environ. Res. Public Health 2021,
18, 8918.
[Google Scholar]
53.
Rinaldi R, De Nucci S, Donghia R, Donvito R, Cerabino N, Di Chito M, et al. Gender Differences in Liver Steatosis and Fibrosis in Overweight and Obese Patients with Metabolic Dysfunction-Associated Steatotic Liver Disease before and after 8 Weeks of Very Low-Calorie Ketogenic Diet.
Nutrients 2024,
16, 1408.
[Google Scholar]
54.
Para O, Crispino P, Barone N, Macis S, Airasca L, Gnerre P, et al. Sex differences in adverse drug reaction and liver disease.
Ital. J. Med. 2018,
12, 15–22.
[Google Scholar]
55.
Straw I, Wu H. Investigating for bias in healthcare algorithms: A sex-stratified analysis of supervised machine learning models in liver disease prediction.
BMJ Health Care Inform. 2022,
29, e100457.
[Google Scholar]
56.
Kardashian A, Serper M, Terrault N, Nephew LD. Health disparities in chronic liver disease.
Hepatology 2023,
77, 1382–1403.
[Google Scholar]
57.
Burra P, Bizzaro D, Gonta A, Shalaby S, Gambato M, Morelli MC, et al. Clinical impact of sexual dimorphism in non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH).
Liver Int. 2021,
41, 1713–1733.
[Google Scholar]
58.
Yang L, Booth C, Speckmann C, Seidel MG, Worth AJJ, Kindle G, et al. Phenotype, genotype, treatment, and survival outcomes in patients with X-linked inhibitor of apoptosis deficiency.
J. Allergy Clin. Immunol. 2022,
150, 456–466.
[Google Scholar]
59.
Holcik M, Korneluk RG. XIAP, the guardian angel.
Nat. Rev. Mol. Cell Biol. 2001,
2, 550–556.
[Google Scholar]
60.
Liston P, Roy N, Tamai K, Lefebvre C, Baird S, Cherton-Horvat G, et al. Suppression of apoptosis in mammalian cells by NAIP and a related family of IAP genes.
Nature 1996,
379, 349–353.
[Google Scholar]
61.
Witt A, Goncharov T, Lee YM, Kist M, Dohse M, Eastham J, et al. XIAP deletion sensitizes mice to TNF-induced and RIP1-mediated death.
Cell Death Dis. 2023,
14, 262.
[Google Scholar]
62.
Kasarinaite A, Sinton M, Saunders PTK, Hay DC. The Influence of Sex Hormones in Liver Function and Disease.
Cells 2023,
12, 1604.
[Google Scholar]
63.
Kaikaew K, Steenbergen J, van Dijk TH, Grefhorst A, Visser JA. Sex Difference in Corticosterone-Induced Insulin Resistance in Mice.
Endocrinology 2019,
160, 2367–2387.
[Google Scholar]
64.
Sarmento-Cabral A, Del Rio-Moreno M, Vazquez-Borrego MC, Mahmood M, Gutierrez-Casado E, Pelke N, et al. GH directly inhibits steatosis and liver injury in a sex-dependent and IGF1-independent manner.
J. Endocrinol. 2021,
248, 31–44.
[Google Scholar]
65.
PubChem Compound Database. Available online: https://www.ncbi.nlm.nih.gov/pccompound/ (accessed on 5 August 2024).
66.
RCSB Protein Data Bank. Available online: http://www.rcsb.org (accessed on 5 August 2024).
67.
Klein SL, Flanagan KL. Sex differences in immune responses.
Nat. Rev. Immunol. 2016,
16, 626–638.
[Google Scholar]
68.
Ma X, Zhou Y, Qiao B, Jiang S, Shen Q, Han Y, et al. Androgen aggravates liver fibrosis by activation of NLRP3 inflammasome in CCl(4)-induced liver injury mouse model.
Am. J. Physiol. Endocrinol. Metab. 2020,
318, E817–E829.
[Google Scholar]
69.
Ali Mondal S, Sathiaseelan R, Mann SN, Kamal M, Luo W, Saccon TD, et al. 17α-estradiol, a lifespan-extending compound, attenuates liver fibrosis by modulating collagen turnover rates in male mice.
Am. J. Physiol. Endocrinol. Metab. 2023,
324, E120–E134.
[Google Scholar]
70.
Mondal SA, Mann SN, van der Linden C, Sathiaseelan R, Kamal M, Das S, et al. Metabolic benefits of 17α-estradiol in liver are partially mediated by ERβ in male mice.
Sci. Rep. 2023,
13, 9841.
[Google Scholar]
71.
Xie G, Wang X, Zhao A, Yan J, Chen W, Jiang R, et al. Sex-dependent effects on gut microbiota regulate hepatic carcinogenic outcomes.
Sci. Rep. 2017,
7, 45232.
[Google Scholar]
72.
Chen XY, Wang C, Huang YZ, Zhang LL. Nonalcoholic fatty liver disease shows significant sex dimorphism.
World J. Clin. Cases 2022,
10, 1457–1472.
[Google Scholar]
73.
Bluemel S, Williams B, Knight R, Schnabl B. Precision medicine in alcoholic and nonalcoholic fatty liver disease via modulating the gut microbiota.
Am. J. Physiol. Gastrointest. Liver Physiol. 2016,
311, G1018–G1036.
[Google Scholar]
74.
Yang M, Qi X, Li N, Kaifi JT, Chen S, Wheeler AA, et al. Western diet contributes to the pathogenesis of non-alcoholic steatohepatitis in male mice via remodeling gut microbiota and increasing production of 2-oleoylglycerol.
Nat. Commun. 2023,
14, 228.
[Google Scholar]
75.
Mauvais-Jarvis F, Bairey Merz N, Barnes PJ, Brinton RD, Carrero JJ, DeMeo DL, et al. Sex and gender: Modifiers of health, disease, and medicine.
Lancet 2020,
396, 565–582.
[Google Scholar]
76.
Ritz SA, Greaves L. Transcending the Male-Female Binary in Biomedical Research: Constellations, Heterogeneity, and Mechanism When Considering Sex and Gender.
Int. J. Environ. Res. Public Health 2022,
19, 4083.
[Google Scholar]
77.
Vasquez-Avila K, Pacheco-Barrios K, de Melo PS, Fregni F. Addressing the critical role of gender identity and sex in the planning, analysis, and conduct of clinical trials.
Princ. Pract. Clin. Res. 2021,
7, 59–62.
[Google Scholar]
78.
Graf J, Simoes E, Kranz A, Weinert K, Abele H. The Importance of Gender-Sensitive Health Care in the Context of Pain, Emergency and Vaccination: A Narrative Review.
Int. J. Environ. Res. Public Health 2023,
21, 13.
[Google Scholar]
79.
Ramos-Lopez O, Milagro FI, Riezu-Boj JI, Martinez JA. Epigenetic signatures underlying inflammation: An interplay of nutrition, physical activity, metabolic diseases, and environmental factors for personalized nutrition.
Inflamm. Res. 2021,
70, 29–49.
[Google Scholar]
80.
Lonardo A, Singal AK, Osna N, Kharbanda KK. Effect of cofactors on NAFLD/NASH and MAFLD. A paradigm illustrating the pathomechanics of organ dysfunction.
Metab. Target Organ Damage 2022,
2, 12.
[Google Scholar]
81.
White AM. Gender Differences in the Epidemiology of Alcohol Use and Related Harms in the United States.
Alcohol. Res. 2020,
40, 01.
[Google Scholar]
82.
Equality EIfG. Gender and Intersecting Inequalities in Access to Health Services 2021. Available online: https://eige.europa.eu/publications-resources/toolkits-guides/gender-equality-index-2021-report/gender-and-intersecting-inequalities-access-health?language_content_entity = en (accessed on 23 September 2024).
83.
Levy M, Chen Y, Clarke R, Guo Y, Lv J, Yu C, et al. Gender differences in use of invasive diagnostic and therapeutic procedures for acute ischaemic heart disease in Chinese adults.
Heart 2022,
108, 292–299.
[Google Scholar]
84.
Maddur H, Shah VH. Alcohol and Liver Function in Women.
Alcohol. Res. 2020,
40, 10.
[Google Scholar]
85.
Bizzaro D, Becchetti C, Trapani S, Lavezzo B, Zanetto A, D’Arcangelo F, et al. Influence of sex in alcohol-related liver disease: Pre-clinical and clinical settings.
United Eur. Gastroenterol. J. 2023,
11, 218–227.
[Google Scholar]
86.
Grant BF, Goldstein RB, Saha TD, Chou SP, Jung J, Zhang H, et al. Epidemiology of DSM-5 Alcohol Use Disorder: Results From the National Epidemiologic Survey on Alcohol and Related Conditions III.
JAMA Psychiatry 2015,
72, 757–766.
[Google Scholar]
87.
Carlini LE, Fernandez AC, Mellinger JL. Sex and gender in alcohol use disorder and alcohol-associated liver disease in the United States: A narrative review. Hepatology 2024. doi:10.1097/HEP.0000000000000905.
88.
Premkumar M, Anand AC. Tobacco, Cigarettes, and the Liver: The Smoking Gun.
J. Clin. Exp. Hepatol. 2021,
11, 700–712.
[Google Scholar]
89.
Balogun O, Wang JY, Shaikh ES, Liu K, Stoyanova S, Memel ZN, et al. Effect of combined tobacco use and type 2 diabetes mellitus on prevalent fibrosis in patients with MASLD.
Hepatol. Commun. 2023,
7, e0300.
[Google Scholar]
90.
She D, Jiang S, Yuan S. Association between serum cotinine and hepatic steatosis and liver fibrosis in adolescent: A population-based study in the United States.
Sci. Rep. 2024,
14, 11424.
[Google Scholar]
91.
Perdomo CM, Frühbeck G, Escalada J. Impact of Nutritional Changes on Nonalcoholic Fatty Liver Disease.
Nutrients 2019,
11, 677.
[Google Scholar]
92.
Wardle J, Haase AM, Steptoe A, Nillapun M, Jonwutiwes K, Bellisle F. Gender differences in food choice: The contribution of health beliefs and dieting.
Ann. Behav. Med. 2004,
27, 107–116.
[Google Scholar]
93.
Calabrò A, Accardi G, Aiello A, Caruso C, Candore G. Sex and gender affect immune aging.
Front. Aging 2023,
4, 1272118.
[Google Scholar]
94.
Petermann-Rocha F, Zhou Z, Mathers JC, Celis-Morales C, Raubenheimer D, Sattar N, et al. Diet modifies the association between alcohol consumption and severe alcohol-related liver disease incidence.
Nat. Commun. 2024,
15, 6880.
[Google Scholar]
95.
Tamargo JA, Sherman KE, Campa A, Martinez SS, Li T, Hernandez J, et al. Food insecurity is associated with magnetic resonance-determined nonalcoholic fatty liver and liver fibrosis in low-income, middle-aged adults with and without HIV.
Am. J. Clin. Nutr. 2021,
113, 593–601.
[Google Scholar]
96.
Tapper EB, Mehta M, Leung CW. Food Insecurity Is Associated With Chronic Liver Disease Among US Adults.
J. Clin. Gastroenterol. 2023,
57, 737–742.
[Google Scholar]
97.
Leung CW, Tapper EB. Food Insecurity is Increasing and is More Common Among Persons with Chronic Liver Disease. Res. Sq. 2024. doi:10.21203/rs.3.rs-4509890/v1.
98.
Prabhakar T, Prasad M, Kumar G, Kaushal K, Shenoy PS, Dubey S, et al. High prevalence of MAFLD in general population: A large cross-sectional study calls for concerted public health action.
Aliment. Pharmacol. Ther. 2024,
59, 843–851.
[Google Scholar]
99.
Straś W, Małkowski P, Tronina O. Hepatocellular carcinoma in patients with non-alcoholic steatohepatitis—Epidemiology, risk factors, clinical implications and treatment.
Clin. Exp. Hepatol. 2020,
6, 170–175.
[Google Scholar]
100.
Craft BB, Carroll HA, Lustyk MK. Gender Differences in Exercise Habits and Quality of Life Reports: Assessing the Moderating Effects of Reasons for Exercise.
Int. J. Lib. Arts Soc. Sci. 2014,
2, 65–76.
[Google Scholar]
101.
Schneider CV, Zandvakili I, Thaiss CA, Schneider KM. Physical activity is associated with reduced risk of liver disease in the prospective UK Biobank cohort.
JHEP Rep. 2021,
3, 100263.
[Google Scholar]
102.
Kim D, Vazquez-Montesino LM, Li AA, Cholankeril G, Ahmed A. Inadequate Physical Activity and Sedentary Behavior Are Independent Predictors of Nonalcoholic Fatty Liver Disease.
Hepatology 2020,
72, 1556–1568.
[Google Scholar]
103.
Sun B, Kang Y, Zhou J, Feng Y, Wang W, Wu X, et al. Association Between Different Types of Physical Activity and Hepatic Steatosis and Liver Fibrosis: A Cross-Sectional Study Based on NHANES. J. Clin. Gastroenterol. 2024. doi:10.1097/MCG.0000000000001985.
104.
Espírito Santo LR, Faria TO, Silva CSO, Xavier LA, Reis VC, Mota GA, et al. Socioeconomic status and education level are associated with dyslipidemia in adults not taking lipid-lowering medication: A population-based study.
Int. Health 2022,
14, 346–353.
[Google Scholar]
105.
Cho IY, Chang Y, Sung E, Kang JH, Wild SH, Byrne CD, et al. Depression and increased risk of non-alcoholic fatty liver disease in individuals with obesity.
Epidemiol. Psychiatr. Sci. 2021,
30, e23.
[Google Scholar]
106.
Lonardo A. The heterogeneity of metabolic syndrome presentation and challenges this causes in its pharmacological management: A narrative review focusing on principal risk modifiers.
Expert Rev. Clin. Pharmacol. 2023,
16, 891–911.
[Google Scholar]
107.
Badini I, Jayaweera K, Pannala G, Adikari A, Siribaddana S, Sumathipala A, et al. Associations between socioeconomic factors and depression in Sri Lanka: The role of gene-environment interplay.
J. Affect. Disord. 2023,
340, 1–9.
[Google Scholar]
108.
Equality EIfG. Health and Risk Behaviours Are Clearly Gendered 2021. Available online: https://eige.europa.eu/publications-resources/toolkits-guides/gender-equality-index-2021-report/health-and-risk-behaviours-are-clearly-gendered?language_content_entity = en (accessed on 19 August 2024).
109.
Thompson AE, Anisimowicz Y, Miedema B, Hogg W, Wodchis WP, Aubrey-Bassler K. The influence of gender and other patient characteristics on health care-seeking behaviour: A QUALICOPC study.
BMC Fam. Pract. 2016,
17, 38.
[Google Scholar]
110.
Das M, Angeli F, Krumeich A, van Schayck OCP. The gendered experience with respect to health-seeking behaviour in an urban slum of Kolkata, India.
Int. J. Equity Health 2018,
17, 24.
[Google Scholar]
111.
Lago-Hernandez C, Nguyen NH, Khera R, Loomba R, Asrani SK, Singh S. Cost-Related Nonadherence to Medications Among US Adults With Chronic Liver Diseases.
Mayo Clin. Proc. 2021,
96, 2639–2650.
[Google Scholar]
112.
Elhence H, Dodge JL, Kahn JA, Lee BP. Characteristics and Outcomes Among US Commercially Insured Transgender Adults With Cirrhosis: A National Cohort Study. Am. J. Gastroenterol. 2024. doi:10.14309/ajg.0000000000002907.
113.
Hashemi L, Marijic Buljubasic A, Budoff MJ, Copeland LA, Jackson NJ, Jasuja GK, et al. Gender-Affirming Hormone Treatment and Metabolic Syndrome Among Transgender Veterans.
JAMA Netw. Open 2024,
7, e2419696.
[Google Scholar]
114.
Deischinger C, Slukova D, Just I, Kaufmann U, Harreiter J, van Trotsenburg M, et al. Effects of gender-affirming hormone therapy on cardiovascular risk factors focusing on glucose metabolism in an Austrian transgender cohort.
Int. J. Transgend. Health 2023,
24, 499–509.
[Google Scholar]
115.
Pothuri VS, Anzelmo M, Gallaher E, Ogunlana Y, Aliabadi-Wahle S, Tan B, et al. Transgender Males on Gender-Affirming Hormone Therapy and Hepatobiliary Neoplasms: A Systematic Review.
Endocr. Pract. 2023,
29, 822–829.
[Google Scholar]
116.
Nikzad N, Fisher AR, Pillai A, Targownik LE, Te HS, Aronsohn A, et al. Considerations in gender-affirming hormone therapy in transgender and gender diverse patients undergoing liver transplantation.
Am. J. Transplant. 2024,
24, 1567–1572.
[Google Scholar]
117.
Pemmasani G, Tremaine WJ, Suresh Kumar VC, Aswath G, Sapkota B, Karagozian R, et al. Sex differences in clinical characteristics and outcomes associated with alcoholic hepatitis.
Eur. J. Gastroenterol. Hepatol. 2023,
35, 1192–1196.
[Google Scholar]
118.
Listabarth S, König D, Berlakovich G, Munda P, Ferenci P, Kollmann D, et al. Sex Disparities in Outcome of Patients with Alcohol-Related Liver Cirrhosis within the Eurotransplant Network-A Competing Risk Analysis.
J. Clin. Med. 2022,
11, 3646.
[Google Scholar]
119.
Chau A, Yeh ML, Tsai PC, Huang DQ, Kim SE, Trinh H, et al. Sex Differences in Treatment Response to Nucleos(t)ide Therapy in Chronic Hepatitis B: A Multicenter Longitudinal Study.
Clin. Gastroenterol. Hepatol. 2024,
22, 572–580.e5.
[Google Scholar]
120.
Duan H, Wang X, Qi W, Shi J, Han L, Wang G, et al. Two genetic variants in the SRD5A2 gene are found to be associated with sex differences in the disease characteristics of patients with chronic hepatitis B virus infection.
Biol. Sex Differ. 2023,
14, 68.
[Google Scholar]
121.
Corsi DJ, Karges W, Thavorn K, Crawley AM, Cooper CL. Influence of female sex on hepatitis C virus infection progression and treatment outcomes.
Eur. J. Gastroenterol. Hepatol. 2016,
28, 405–411.
[Google Scholar]
122.
Grattagliano I, Rossi A, Marconi E, Lapi F, Cricelli C. Determinants of HCV-related complications in Italian primary care patients.
Liver Int. 2021,
41, 2857–2865.
[Google Scholar]
123.
Lonardo A, Nascimbeni F, Ballestri S, Fairweather D, Win S, Than TA, et al. Sex Differences in Nonalcoholic Fatty Liver Disease: State of the Art and Identification of Research Gaps.
Hepatology 2019,
70, 1457–1469.
[Google Scholar]
124.
Balakrishnan M, Patel P, Dunn-Valadez S, Dao C, Khan V, Ali H, et al. Women Have a Lower Risk of Nonalcoholic Fatty Liver Disease but a Higher Risk of Progression vs Men: A Systematic Review and Meta-analysis.
Clin. Gastroenterol. Hepatol. 2021,
19, 61–71.e15.
[Google Scholar]
125.
Pérez-Montes de Oca A, Julián MT, Pera G, Caballería L, Morillas R, Torán P, et al. Dysglycemia in young women attenuates the protective effect against fatty liver disease.
Front. Endocrinol. 2022,
13, 971864.
[Google Scholar]
126.
Ciardullo S, Oltolini A, Cannistraci R, Muraca E, Perseghin G. Sex-related association of nonalcoholic fatty liver disease and liver fibrosis with body fat distribution in the general US population.
Am. J. Clin. Nutr. 2022,
115, 1528–1534.
[Google Scholar]
127.
Yan LJ, Yao SY, Meng GX, Liu KX, Li HC, Ding ZN, et al. Sex and regional disparities in incidence of hepatocellular carcinoma in autoimmune hepatitis: A systematic review and meta-analysis.
Hepatol. Int. 2021,
15, 1413–1420.
[Google Scholar]
128.
Wu YH, Chiu YL, Lin JC, Chen HW. New insights into sex differences in primary biliary cholangitis. Gender difference in primary biliary cholangitis.
J. Pak. Med. Assoc. 2022,
72, 896–900.
[Google Scholar]
129.
Abdulkarim M, Zenouzi R, Sebode M, Schulz L, Quaas A, Lohse AW, et al. Sex differences in clinical presentation and prognosis in patients with primary biliary cholangitis.
Scand. J. Gastroenterol. 2019,
54, 1391–1396.
[Google Scholar]
130.
Xiong YT, Wang JF, Niu XX, Fu YM, Wang KX, Wang CY, et al. Autoimmunity associates with severity of illness in elderly patients with drug-induced liver injury.
Front. Pharmacol. 2023,
14, 1071709.
[Google Scholar]
131.
Nunes D, Breton MC, Monteiro CSJ, Dos Santos JL. Drug Induced Liver Injury: Perspective of the Adverse Drug Reaction Reports to the Portuguese Pharmacovigilance System from 2010 to 2019.
Healthcare 2021,
9, 1630.
[Google Scholar]
132.
Wang CY, Deng Y, Li P, Zheng S, Chen G, Zhou G, et al. Prediction of biochemical nonresolution in patients with chronic drug-induced liver injury: A large multicenter study.
Hepatology 2022,
75, 1373–1385.
[Google Scholar]
133.
Addolorato G, Abenavoli L, Dallio M, Federico A, Germani G, Gitto S, et al. Alcohol associated liver disease 2020: A clinical practice guideline by the Italian Association for the Study of the Liver (AISF).
Dig Liver Dis. 2020,
52, 374–391.
[Google Scholar]
134.
Aslam A, Kwo PY. Epidemiology and Disease Burden of Alcohol Associated Liver Disease.
J. Clin. Exp. Hepatol. 2023,
13, 88–102.
[Google Scholar]
135.
Osna NA, Donohue TM, Jr., Kharbanda KK. Alcoholic Liver Disease: Pathogenesis and Current Management.
Alcohol. Res. 2017,
38, 147–161.
[Google Scholar]
136.
Han S, Yang Z, Zhang T, Ma J, Chandler K, Liangpunsakul S. Epidemiology of Alcohol-Associated Liver Disease.
Clin. Liver Dis. 2021,
25, 483–492.
[Google Scholar]
137.
Sayaf K, Gabbia D, Russo FP, De Martin S. The Role of Sex in Acute and Chronic Liver Damage.
Int. J. Mol. Sci. 2022,
23, 10654.
[Google Scholar]
138.
Toniutto P, Shalaby S, Mameli L, Morisco F, Gambato M, Cossiga V, et al. Role of sex in liver tumor occurrence and clinical outcomes: A comprehensive review.
Hepatology 2024,
79, 1141–1157.
[Google Scholar]
139.
Gao B, Zeng S, Maccioni L, Shi X, Armando A, Quehenberger O, et al. Lipidomics for the Prediction of Progressive Liver Disease in Patients with Alcohol Use Disorder.
Metabolites 2022,
12, 433.
[Google Scholar]
140.
Mackowiak B, Fu Y, Maccioni L, Gao B. Alcohol-associated liver disease. J. Clin. Investig. 2024, 134.
141.
Foundation HB. Hepatitis B Facts and Figures 2024. Available online: https://www.hepb.org/what-is-hepatitis-b/what-is-hepb/facts-and-figures/#:~:text = Hepatitis%20B%20Around%20the%20World, million%20people%20are%20chronically%20infected (accessed on 15 September 2024).
142.
Wang SH, Chen PJ, Yeh SH. Gender disparity in chronic hepatitis B: Mechanisms of sex hormones.
J. Gastroenterol. Hepatol. 2015,
30, 1237–1245.
[Google Scholar]
143.
Chu CM, Liaw YF, Sheen IS, Lin DY, Huang MJ. Sex difference in chronic hepatitis B virus infection: An appraisal based on the status of hepatitis B e antigen and antibody.
Hepatology 1983,
3, 947–950.
[Google Scholar]
144.
Su FH, Chen JD, Cheng SH, Lin CH, Liu YH, Chu FY. Seroprevalence of Hepatitis-B infection amongst Taiwanese university students 18 years following the commencement of a national Hepatitis-B vaccination program.
J. Med. Virol. 2007,
79, 138–143.
[Google Scholar]
145.
Chen CJ, Yang HI, Iloeje UH. Hepatitis B virus DNA levels and outcomes in chronic hepatitis B.
Hepatology 2009,
49 (5 Suppl), S72–S84.
[Google Scholar]
146.
Esmaeili A, Mirzazadeh A, Morris MD, Hajarizadeh B, Sacks HS, Maher L, et al. The Effect of Female Sex on Hepatitis C Incidence Among People Who Inject Drugs: Results From the International Multicohort InC3 Collaborative.
Clin. Infect. Dis. 2018,
66, 20–28.
[Google Scholar]
147.
Zhou S, Qi K, Bersoff-Matcha SJ, Mishra P, Struble K. Sex-related difference analyses of efficacy and safety in clinical trials of direct-acting antivirals to treat chronic HCV genotype 1 and 3 infections.
J. Viral Hepat. 2024,
31, 78–87.
[Google Scholar]
148.
Li J, Gordon SC, Zhou Y, Boscarino JA, Schmidt MA, Daida YG, et al. Sex Differences in Extrahepatic Outcomes After Antiviral Treatment for Hepatitis C.
Am. J. Gastroenterol. 2021,
116, 576–583.
[Google Scholar]
149.
Ruggieri A, Gagliardi MC, Anticoli S. Sex-Dependent Outcome of Hepatitis B and C Viruses Infections: Synergy of Sex Hormones and Immune Responses?
Front. Immunol. 2018,
9, 2302.
[Google Scholar]
150.
Cherubini A, Della Torre S, Pelusi S, Valenti L. Sexual dimorphism of metabolic dysfunction-associated steatotic liver disease. Trends Mol. Med. 2024. doi:10.1016/j.molmed.2024.05.013.
151.
Ballestri S, Nascimbeni F, Baldelli E, Marrazzo A, Romagnoli D, Lonardo A. NAFLD as a Sexual Dimorphic Disease: Role of Gender and Reproductive Status in the Development and Progression of Nonalcoholic Fatty Liver Disease and Inherent Cardiovascular Risk.
Adv. Ther. 2017,
34, 1291–1326.
[Google Scholar]
152.
Lonardo A, Bellentani S, Argo CK, Ballestri S, Byrne CD, Caldwell SH, et al. Epidemiological modifiers of non-alcoholic fatty liver disease: Focus on high-risk groups.
Dig. Liver Dis. 2015,
47, 997–1006.
[Google Scholar]
153.
Cherubini A, Ostadreza M, Jamialahmadi O, Pelusi S, Rrapaj E, Casirati E, et al. Interaction between estrogen receptor-α and PNPLA3 p.I148M variant drives fatty liver disease susceptibility in women.
Nat. Med. 2023,
29, 2643–2655.
[Google Scholar]
154.
Della Torre S, Cherubini A, Valenti L. Estrogen receptor alpha in the female liver: Dr. Jekyll and Mr. Hyde.
J. Hepatol. 2024,
81, 763–765.
[Google Scholar]
155.
Booijink R, Ramachandran P, Bansal R. Implications of innate immune sexual dimorphism for MASLD pathogenesis and treatment.
Trends Pharmacol. Sci. 2024,
45, 614–627.
[Google Scholar]
156.
Xin G, Qin S, Wang S, Wang X, Zhang Y, Wang J. Sex hormone affects the severity of non-alcoholic steatohepatitis through the MyD88-dependent IL-6 signaling pathway.
Exp. Biol. Med. 2015,
240, 1279–1286.
[Google Scholar]
157.
Pellicano R, Ferro A, Cicerchia F, Mattivi S, Fagoonee S, Durazzo M. Autoimmune Hepatitis and Fibrosis.
J. Clin. Med. 2023,
12, 1979.
[Google Scholar]
158.
Guy J, Peters MG. Liver disease in women: The influence of gender on epidemiology, natural history, and patient outcomes.
Gastroenterol. Hepatol. 2013,
9, 633–639.
[Google Scholar]
159.
Pemberton PW, Aboutwerat A, Smith A, Burrows PC, McMahon RF, Warnes TW. Oxidant stress in type I autoimmune hepatitis: The link between necroinflammation and fibrogenesis?
Biochim. Biophys. Acta 2004,
1689, 182–189.
[Google Scholar]
160.
Torrens-Mas M, Pons DG, Sastre-Serra J, Oliver J, Roca P. Sexual hormones regulate the redox status and mitochondrial function in the brain. Pathological Implications.
Redox Biol. 2020,
31, 101505.
[Google Scholar]
161.
Ismail A, Kennedy L, Francis H. Sex-Dependent Differences in Cholestasis: Why Estrogen Signaling May Be a Key Pathophysiological Driver.
Am. J. Pathol. 2023,
193, 1355–1362.
[Google Scholar]
162.
Colapietro F, Bertazzoni A, Lleo A. Contemporary Epidemiology of Primary Biliary Cholangitis.
Clin. Liver Dis. 2022,
26, 555–570.
[Google Scholar]
163.
Tanaka A, Ma X, Takahashi A, Vierling JM. Primary biliary cholangitis.
Lancet 2024,
404, 1053–1066.
[Google Scholar]
164.
Dyson JK, Beuers U, Jones DEJ, Lohse AW, Hudson M. Primary sclerosing cholangitis.
Lancet 2018,
391, 2547–2559.
[Google Scholar]
165.
Erasmus HP, Bektas R, Orland K, Trifonova S, Gu WY, Uschner FE, et al. Variceal bleeding has increased mortality compared to nonvariceal bleeding only in males.
Eur. J. Gastroenterol. Hepatol. 2021,
33 (1S Suppl 1), e94–e101.
[Google Scholar]
166.
Lee DU, Kwon J, Han J, Chang K, Kolachana S, Bahadur A, et al. The Impact of Race and Sex on the Clinical Outcomes of Homeless Patients With Alcoholic Liver Disease: Propensity Score Matched Analysis of US Hospitals.
J. Clin. Gastroenterol. 2024,
58, 708–717.
[Google Scholar]
167.
Degasperi E, D’Ambrosio R, Iavarone M, Sangiovanni A, Aghemo A, Soffredini R, et al. Factors Associated With Increased Risk of De Novo or Recurrent Hepatocellular Carcinoma in Patients With Cirrhosis Treated With Direct-Acting Antivirals for HCV Infection.
Clin. Gastroenterol. Hepatol. 2019,
17, 1183–1191.e7.
[Google Scholar]
168.
Ladenheim MR, Kim NG, Nguyen P, Le A, Stefanick ML, Garcia G, et al. Sex differences in disease presentation, treatment and clinical outcomes of patients with hepatocellular carcinoma: A single-centre cohort study.
BMJ Open Gastroenterol. 2016,
3, e000107.
[Google Scholar]
169.
Huang J, Wei S, Tang Y, Zhang Q, Luo H, Tang Z, et al. Sex Differences in the Impact of Metabolic Dysfunction-associated Fatty Liver Disease on the of Patients with Hepatocellular Carcinoma after Radical Resection.
J. Cancer 2023,
14, 1107–1116.
[Google Scholar]
170.
De la Cruz Ku G, Aizpuru M, Hackl H, Ubl DS, Habermann EB, Pery R, et al. Hepatocellular carcinoma as predominant cancer subgroup accounting for sex differences in post-hepatectomy liver failure, morbidity and mortality.
HPB 2022,
24, 1453–1463.
[Google Scholar]
171.
Lonardo A, Ballestri S, Chow PKH, Suzuki A. Sex disparity in hepatocellular carcinoma owing to NAFLD and non-NAFLD etiology: Epidemiological findings and pathobiological mechanisms.
Hepatoma Res. 2020,
6, 83.
[Google Scholar]
172.
Lugari S, Baldelli E, Lonardo A. Metabolic primary liver cancer in adults: Risk factors and pathogenic mechanisms.
Metab. Target Organ Damage 2023,
3, 5.
[Google Scholar]
173.
Lee C, Jung Y. Sex disparity in the liver regeneration focusing on sex hormones. Metab.
Target Organ Damage 2023,
3, 10.
[Google Scholar]
174.
Lonardo A. Is liver fibrosis a risk factor for gynecological cancers?
Metab. Target Organ Damage 2024,
4, 7.
[Google Scholar]
175.
Mantovani A, Lonardo A, Stefan N, Targher G. Metabolic dysfunction-associated steatotic liver disease and extrahepatic gastrointestinal cancers.
Metabolism 2024,
160, 156014.
[Google Scholar]
176.
Guarino M, Cossiga V, Becchetti C, Invernizzi F, Lapenna L, Lavezzo B, et al. Sarcopenia in chronic advanced liver diseases: A sex-oriented analysis of the literature.
Dig. Liver Dis. 2022,
54, 997–1006.
[Google Scholar]
177.
Anderson LJ, Liu H, Garcia JM. Sex Differences in Muscle Wasting.
Adv. Exp. Med. Biol. 2017,
1043, 153–197.
[Google Scholar]
178.
Ren X, Hao S, Yang C, Yuan L, Zhou X, Zhao H, et al. Alterations of intestinal microbiota in liver cirrhosis with muscle wasting.
Nutrition 2021,
83, 111081.
[Google Scholar]
179.
Li X, He J, Sun Q. The prevalence and effects of sarcopenia in patients with metabolic dysfunction-associated steatotic liver disease (MASLD): A systematic review and meta-analysis.
Clin. Nutr. 2024,
43, 2005–2016.
[Google Scholar]
180.
Fozouni L, Wang CW, Lai JC. Sex Differences in the Association Between Frailty and Sarcopenia in Patients With Cirrhosis.
Clin. Transl. Gastroenterol. 2019,
10, e00102.
[Google Scholar]
181.
Mantovani A, Csermely A, Tilg H, Byrne CD, Targher G. Comparative effects of non-alcoholic fatty liver disease and metabolic dysfunction-associated fatty liver disease on risk of incident cardiovascular events: A meta-analysis of about 13 million individuals.
Gut 2023,
72, 1433–1436.
[Google Scholar]
182.
Mantovani A, Csermely A, Petracca G, Beatrice G, Corey KE, Simon TG, et al. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: An updated systematic review and meta-analysis.
Lancet Gastroenterol. Hepatol. 2021,
6, 903–913.
[Google Scholar]
183.
Choe HJ, Moon JH, Kim W, Koo BK, Cho NH. Steatotic liver disease predicts cardiovascular disease and advanced liver fibrosis: A community-dwelling cohort study with 20-year follow-up.
Metabolism 2024,
153, 155800.
[Google Scholar]
184.
Wang SW, Hsieh TH, Cheng YM, Wang CC, Kao JH. Liver and atherosclerotic risks of patients with cryptogenic steatotic liver disease.
Hepatol. Int. 2024,
18, 943–951.
[Google Scholar]
185.
Ren R, Zheng Y. Sex differences in cardiovascular and all-cause mortality in nonalcoholic fatty liver disease in the US population.
Nutr. Metab. Cardiovasc. Dis. 2023,
33, 1349–1357.
[Google Scholar]
186.
Wang J, Lonardo A. Commentary: Of women, liver, and heart.
Metab. Target Organ Damage 2023,
3, 14.
[Google Scholar]
187.
Parikh NS, Koh I, VanWagner LB, Elkind MSV, Zakai NA, Cushman M. Liver Fibrosis is Associated with Ischemic Stroke Risk in Women but not Men: The REGARDS Study.
J. Stroke Cerebrovasc. Dis. 2021,
30, 105788.
[Google Scholar]
188.
Kautzky-Willer A, Leutner M, Harreiter J. Sex differences in type 2 diabetes.
Diabetologia 2023,
66, 986–1002.
[Google Scholar]
189.
Lonardo A, Ballestri S, Guaraldi G, Nascimbeni F, Romagnoli D, Zona S, et al. Fatty liver is associated with an increased risk of diabetes and cardiovascular disease—Evidence from three different disease models: NAFLD, HCV and HIV.
World J. Gastroenterol. 2016,
22, 9674–9693.
[Google Scholar]
190.
Guaraldi G, Lonardo A, Ballestri S, Zona S, Stentarelli C, Orlando G, et al. Human immunodeficiency virus is the major determinant of steatosis and hepatitis C virus of insulin resistance in virus-associated fatty liver disease.
Arch. Med. Res. 2011,
42, 690–697.
[Google Scholar]
191.
Mantovani A, Petracca G, Beatrice G, Tilg H, Byrne CD, Targher G. Non-alcoholic fatty liver disease and risk of incident diabetes mellitus: An updated meta-analysis of 501 022 adult individuals.
Gut 2021,
70, 962–969.
[Google Scholar]
192.
Mantovani A, Petracca G, Beatrice G, Csermely A, Lonardo A, Schattenberg JM, et al. Non-alcoholic fatty liver disease and risk of incident chronic kidney disease: An updated meta-analysis.
Gut 2022,
71, 156–162.
[Google Scholar]
193.
Lonardo A, Mantovani A, Targher G, Baffy G. Nonalcoholic Fatty Liver Disease and Chronic Kidney Disease: Epidemiology, Pathogenesis, and Clinical and Research Implications.
Int. J. Mol. Sci. 2022,
23, 13320.
[Google Scholar]
194.
Agustanti N, Soetedjo NNM, Damara FA, Iryaningrum MR, Permana H, Bestari MB, et al. The association between metabolic dysfunction-associated fatty liver disease and chronic kidney disease: A systematic review and meta-analysis.
Diabetes Metab. Syndr. 2023,
17, 102780.
[Google Scholar]
195.
Lonardo A. Association of NAFLD/NASH, and MAFLD/MASLD with chronic kidney disease: An updated narrative review.
Metab. Target Organ Damage 2024,
4, 16.
[Google Scholar]
196.
Adrian T, Hornum M, Knop FK, Christensen KB, Almdal T, Rossing P, et al. Hepatic Fibrosis Evaluated in Patients with Type 2 Diabetes with and without Chronic Kidney Disease.
Nephron 2023,
147, 673–684.
[Google Scholar]
197.
Marc L, Mihaescu A, Lupusoru R, Grosu I, Gadalean F, Bob F, et al. Liver Steatosis: Better Predictor of CKD in MAFLD Than Liver Fibrosis as Determined by Transient Elastography With Controlled Attenuation Parameter.
Front. Med. 2021,
8, 788881.
[Google Scholar]
198.
Argo CK, Northup PG, Al-Osaimi AM, Caldwell SH. Systematic review of risk factors for fibrosis progression in non-alcoholic steatohepatitis.
J. Hepatol. 2009,
51, 371–379.
[Google Scholar]
199.
Shen Y, Cai R, Sun J, Dong X, Huang R, Tian S, et al. Diabetes mellitus as a risk factor for incident chronic kidney disease and end-stage renal disease in women compared with men: A systematic review and meta-analysis.
Endocrine 2017,
55, 66–76.
[Google Scholar]
200.
Arnold AP, Klein SL, McCarthy MM, Mogil JS. Male-female comparisons are powerful in biomedical research—don’t abandon them.
Nature 2024,
629, 37–40.
[Google Scholar]
201.
Weldegiorgis M, Woodward M. The impact of hypertension on chronic kidney disease and end-stage renal disease is greater in men than women: A systematic review and meta-analysis.
BMC Nephrol. 2020,
21, 506.
[Google Scholar]
202.
Lima-Posada I, Bobadilla NA. Understanding the opposite effects of sex hormones in mediating renal injury.
Nephrology 2021,
26, 217–226.
[Google Scholar]
203.
Kittikulsuth W, Sullivan JC, Pollock DM. ET-1 actions in the kidney: Evidence for sex differences.
Br. J. Pharmacol. 2013,
168, 318–326.
[Google Scholar]
204.
Yen P-C, Chou Y-T, Li C-H, Sun Z-J, Wu C-H, Chang Y-F, et al. Hyperuricemia Is Associated with Significant Liver Fibrosis in Subjects with Nonalcoholic Fatty Liver Disease, but Not in Subjects without It.
J. Clin. Med. 2022,
11, 1445.
[Google Scholar]
205.
Wang CY, Kao HH, Lai KY, Lin CC, Lin WY, Liu CS, et al. Clinical and Metabolic Characteristics of Hyperuricemia with Risk of Liver Fibrosis: A Cross-Sectional Study.
Metabolites 2022,
12, 893.
[Google Scholar]
206.
Lee JM, Kim HW, Heo SY, Do KY, Lee JD, Han SK, et al. Associations of Serum Uric Acid Level With Liver Enzymes, Nonalcoholic Fatty Liver Disease, and Liver Fibrosis in Korean Men and Women: A Cross-Sectional Study Using Nationally Representative Data.
J. Korean Med. Sci. 2023,
38, e267.
[Google Scholar]
207.
Jaruvongvanich V, Ahuja W, Wijarnpreecha K, Ungprasert P. Hyperuricemia is not associated with severity of liver fibrosis in patients with nonalcoholic fatty liver disease: A systematic review and meta-analysis.
Eur. J. Gastroenterol. Hepatol. 2017,
29, 694–697.
[Google Scholar]
208.
Halperin Kuhns VL, Woodward OM. Sex Differences in Urate Handling.
Int. J. Mol. Sci. 2020,
21, 4269.
[Google Scholar]
209.
Murata A, Hyogo H, Nonaka M, Sumioka A, Suehiro Y, Furudoi A, et al. Overlooked muscle cramps in patients with chronic liver disease: In relation to the prevalence of muscle cramps.
Eur. J. Gastroenterol. Hepatol. 2019,
31, 375–381.
[Google Scholar]
210.
Labenz C, Kostev K, Kaps L, Galle PR, Schattenberg JM. Incident Dementia in Elderly Patients with Nonalcoholic Fatty Liver Disease in Germany.
Dig. Dis. Sci. 2021,
66, 3179–3185.
[Google Scholar]
211.
Shang Y, Nasr P, Ekstedt M, Widman L, Stål P, Hultcrantz R, et al. Non-alcoholic fatty liver disease does not increase dementia risk although histology data might improve risk prediction.
JHEP Rep. 2021,
3, 100218.
[Google Scholar]
212.
Shang Y, Widman L, Hagström H. Nonalcoholic Fatty Liver Disease and Risk of Dementia: A Population-Based Cohort Study.
Neurology 2022,
99, e574–e582.
[Google Scholar]
213.
Xiao T, van Kleef LA, Ikram MK, de Knegt RJ, Ikram MA. Association of Nonalcoholic Fatty Liver Disease and Fibrosis With Incident Dementia and Cognition: The Rotterdam Study.
Neurology 2022,
99, e565–e573.
[Google Scholar]
214.
Jeong S, Oh YH, Choi S, Chang J, Kim SM, Son JS, et al. Association of non-alcoholic fatty liver disease with incident dementia later in life among elder adults.
Clin. Mol. Hepatol. 2022,
28, 510–521.
[Google Scholar]
215.
Weinstein G, O’Donnell A, Frenzel S, Xiao T, Yaqub A, Yilmaz P, et al. Nonalcoholic fatty liver disease, liver fibrosis, and structural brain imaging: The Cross-Cohort Collaboration.
Eur. J. Neurol. 2024,
31, e16048.
[Google Scholar]
216.
Lu Y, Pike JR, Hoogeveen RC, Walker KA, Raffield LM, Selvin E, et al. Liver integrity and the risk of Alzheimer’s disease and related dementias.
Alzheimers Dement. 2024,
20, 1913–1922.
[Google Scholar]
217.
Li YS, Xia YG, Liu YL, Jiang WR, Qiu HN, Wu F, et al. Metabolic-dysfunction associated steatotic liver disease-related diseases, cognition and dementia: A two-sample mendelian randomization study.
PLoS ONE 2024,
19, e0297883.
[Google Scholar]
218.
Weinstein G, Schonmann Y, Yeshua H, Zelber-Sagi S. The association between liver fibrosis score and incident dementia: A nationwide retrospective cohort study.
Alzheimers Dement. 2024,
20, 5385–5397.
[Google Scholar]
219.
Parikh NS, Kamel H, Zhang C, Kumar S, Rosenblatt R, Spincemaille P, et al. Association between liver fibrosis and incident dementia in the UK Biobank study.
Eur. J. Neurol. 2022,
29, 2622–2630.
[Google Scholar]
220.
Wang YR, Wang QH, Zhang T, Liu YH, Yao XQ, Zeng F, et al. Associations Between Hepatic Functions and Plasma Amyloid-Beta Levels-Implications for the Capacity of Liver in Peripheral Amyloid-Beta Clearance.
Mol. Neurobiol. 2017,
54, 2338–2344.
[Google Scholar]
221.
Kershenobich Stalnikowitz D, Weissbrod AB. Liver fibrosis and inflammation. A review.
Ann. Hepatol. 2003,
2, 159–163.
[Google Scholar]
222.
Walker KA, Power MC, Hoogeveen RC, Folsom AR, Ballantyne CM, Knopman DS, et al. Midlife Systemic Inflammation, Late-Life White Matter Integrity, and Cerebral Small Vessel Disease: The Atherosclerosis Risk in Communities Study.
Stroke 2017,
48, 3196–3202.
[Google Scholar]
223.
Boursier J, Mueller O, Barret M, Machado M, Fizanne L, Araujo-Perez F, et al. The severity of nonalcoholic fatty liver disease is associated with gut dysbiosis and shift in the metabolic function of the gut microbiota.
Hepatology 2016,
63, 764–775.
[Google Scholar]
224.
De Minicis S, Rychlicki C, Agostinelli L, Saccomanno S, Candelaresi C, Trozzi L, et al. Dysbiosis contributes to fibrogenesis in the course of chronic liver injury in mice.
Hepatology 2014,
59, 1738–1749.
[Google Scholar]
225.
Nicoletti A, Ponziani FR, Biolato M, Valenza V, Marrone G, Sganga G, et al. Intestinal permeability in the pathogenesis of liver damage: From non-alcoholic fatty liver disease to liver transplantation.
World J. Gastroenterol. 2019,
25, 4814–4834.
[Google Scholar]
226.
Ferreiro AL, Choi J, Ryou J, Newcomer EP, Thompson R, Bollinger RM, et al. Gut microbiome composition may be an indicator of preclinical Alzheimer’s disease.
Sci. Transl. Med. 2023,
15, eabo2984.
[Google Scholar]
227.
You SC, Kim KJ, Kim SU, Kim BK, Park JY, Kim DY, et al. Hepatic fibrosis assessed using transient elastography independently associated with coronary artery calcification.
J. Gastroenterol. Hepatol. 2015,
30, 1536–1542.
[Google Scholar]
228.
Jamalinia M, Zare F, Lankarani KB. Systematic review and meta-analysis: Association between liver fibrosis and subclinical atherosclerosis in nonalcoholic fatty liver disease.
Aliment. Pharmacol. Ther. 2023,
58, 384–394.
[Google Scholar]
229.
Petta S, Tuttolomondo A, Gagliardo C, Zafonte R, Brancatelli G, Cabibi D, et al. The Presence of White Matter Lesions Is Associated With the Fibrosis Severity of Nonalcoholic Fatty Liver Disease.
Medicine 2016,
95, e3446.
[Google Scholar]
230.
Xiong S, Yin S, Deng W, Zhao Y, Li W, Wang P, et al. Impact of liver fibrosis score on the incidence of stroke: A cohort study.
Liver Int. 2022,
42, 2175–2185.
[Google Scholar]