Article Open Access
Received: 25 April 2024 Accepted: 24 June 2024 Published: 02 July 2024

© 2024 The authors. This is an open access article under the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/).
In the last decennia, various studies have reported high prevalence of psychiatric disorders in children/adolescents , young adults and adults with intellectual disabilities (ID) [1,2,3,4,5,6,7,8,9,10,11,12,13]. For example, a study by Dekker and Koot [4] showed that 21.9% of the 474 children and adolescents with ID in their sample met the DSM-IV symptom criteria for anxiety disorder, 4.4% for mood disorder, and 25.1% for disruptive disorder. More than half of those meeting the criteria for a DSM-IV disorder were severely impaired in everyday functioning, and about 37% had a comorbid disorder. Further, studies also reported high stability of psychopathology from childhood into adulthood in individuals with ID [14]. Therefore, it seems essential to prevent the development of these problems as early as possible. However, so far, only a few studies addressed risk factors for psychiatric disorders in youth with ID using a prospective design. Therefore, hardly anything is known on factors to be targeted in efforts to prevent these disorders. The goals of this study were to identify risk indicators present at ages 6–18 associated with DSM-IV diagnoses five years later and to assess the potential health gain and efficiency of preventive interventions targeting these risk indicators.
The development of psychopathology in youths with ID in the context of risk may be understood from a general developmental framework. The bioecological model of human development [15] offers a holistic approach to analysing the influences of child-related and environmental factors on the child’s development. According to this model, factors at the microsystem level, including factors at the family level, have the most influence on the child, next to influences from child characteristics. We assume that mechanisms and factors explaining the development of children and adolescents from the general population apply equally to populations of youths with ID and equally apply to the development of psychiatric problems. For example, studies on risk and adversity in developmental psychopathology [16] have identified factors like previous psychopathology of the child, (chronic) physical condition, learning problems, stressful life events, maternal psychopathology, family dysfunction, and low socioeconomic status as risk factors. Over and above these, limitations in cognitive and social skills may pose additional risk for children and adolescents with ID. This study focuses on each of these factors.
Studies in the general population have found elevated levels of emotional and behavioural problems and psychiatric disorders in childhood to be predictive of the onset and continuity of psychiatric disorders in adolescence and adulthood [17]. Besides childhood psychopathology, also gender, social competence, self-esteem, chronic physical illness of the child or parent, socio-economical status, ethnicity, early adverse life-experiences, and family structure and functioning have been found to be prospectively associated with psychiatric disorders [17,18,19,20,21,22,23].
While the co-occurrence of ID and mental health problems in children and adolescents has been well-documented [6,24,25], very little research has addressed the association between a range of risk factors and mental health issues in this population. Most studies address the association of specific experiences (e.g., maltreatment) with specific outcomes (e.g., depression), although some efforts are made for broader perspectives using cross-sectional study designs. For example, Weiss, Ting, and Perry [26] found that youth with a psychiatric diagnosis had higher levels of adaptive behavior and experienced more negative life events than youth without a psychiatric diagnosis, while the presence of clinically significant maladaptive behavior was related to higher levels of adaptive behavior, parents’ mental health problems and lower family quality of life. Whitney et al. [27] showed that co-morbid conditions, physical and social factors, autism spectrum disorders, Down syndrome, attention-deficit/hyperactivity disorder, pain, and bully victimisation were each associated with depression and/or anxiety problems. However, very little has been done to address prospective relations between risk and mental health outcomes in this population, and in fact, many longitudinal epidemiological studies of prevalence, risk factors, and continuity/discontinuity of child and adolescent mental disorders omitted study participants with ID/IDD [28].
Only a few studies identified factors associated with psychiatric disorders among people with ID. In a study among children and adolescents with mild to moderate ID, apart from initial high levels of problem behaviour, child low social competence, inadequate daily living skills, child health problems, negative life events, parental psychopathology, and poor family functioning were found to be predictive of DSM-IV diagnoses one year later [29]. Significant associations between psychopathology and the experience of negative life events were demonstrated in cross-sectional studies among adults [30,31] and children with ID [32]. A longitudinal study by McCarthy and Boyd [33] among people with Down’s syndrome, however, found no significant associations between childhood levels of adaptive behaviour, or family factors like social class or parental psychopathology, and psychiatric disorders in adulthood.
The studies described above successfully identified high-risk groups of children but also had several limitations. They predominantly focussed on clinical samples, samples of children or adults with ID in residential settings, or people with a specific syndrome, and most studies only looked at cross-sectional or short term longitudinal associations between psychopathology and child/adolescent risk factors. The first aim of this study is to identify child/adolescent risk indicators of psychiatric problems of individuals identified in adolescence or young adulthood. The study takes a prospective longitudinal approach tracking children and adolescents with ID across a five-year period. The transitional periods from childhood to adolescence and adolescence to young adulthood are of special interest as these periods put increasing demands on these individuals and their families in several important life domains, including social relations, education, and possibly entrance into the labour market. Especially normative demands involving independence and participation in society require more adaptation than may be expected given the limitations of young people with ID. Across these periods, in the general population, serious symptoms of depression and conduct tend to rise (specifically in females and males, respectively), and other problems (e.g., anxiety) tend to grow into more serious forms (e.g., from separation anxiety into social anxiety). However, the extant knowledge on the contribution of personal and family factors to the development of psychiatric problems in children and adolescents with ID across the transition to adolescence and young adulthood, respectively, is seriously wanting.
As demonstrated by several studies in clinical as well as general population samples, child/adolescent psychopathology tends to be fairly stable, and psychiatric disorders show fairly high levels of continuity, also in individuals with ID [14]. Therefore, there is a strong need to prevent the development of psychiatric problems in children/adolescents with ID and identify malleable risk factors related to this development. However, we are unaware of any study that empirically addressed that need. From a prevention perspective, several indices are informative about the potency of reduction of psychiatric problems when specific risk factors are tackled successfully. First, the impact of risk factors on the development of psychiatric disorders tells us how big the chance is for a child who is exposed to a certain risk factor to develop a certain psychiatric disorder. Exposure to some risk factors might have a larger impact than exposure to other risk factors. Risk factors with a larger impact should be the focus of preventive strategies. The impact of risk factors can be described by the risk difference (RD) index, which is the difference in the risk of developing a psychiatric problem between exposed and unexposed children/adolescents. Its inverse, the number needed to be treated (NNT) indicates how many children/adolescents would have to receive a preventive intervention to avoid one new case with psychiatric problems, assuming that the adverse effect of the risk factor can be completely blocked by some preventive intervention. The NNT is thus an indicator of the maximum efficiency of the intervention. To assess the potential health gain in a population the incidence rate ratio (IRR) and the attributable fraction (AF) are useful. The IRR is the ratio of the incidence rate of psychiatric problems in a group of exposed children over the incidence rate in the unexposed group. The IRR thus captures the strength of association between an exposure and outcome, not unlike a relative risk or an odds ratio. Finally, the AF reflects the percentage by which the incidence rate of psychiatric problems can be reduced when the adverse effect of a risk factor is eliminated by a preventive intervention. Higher RDs, IRRs, and AFs, and lower NNTs point to greater utility of the studied risk indicators for preventive interventions because then we may expect that substantial health gains can be generated efficiently.
The second aim of this study is to evaluate the impact, efficiency, and possible health gain of addressing risk factors associated with psychiatric problems in adolescents and young adults with ID. This epidemiological approach recently introduced in the area of adult depression [34,35] and applied in the field of childhood internalising problems [36], was expected to throw some light on potential preventive intervention targets related to these psychiatric problems.
Not only is it necessary to identify risk indicators for the development of psychiatric disorders and their relevance in preventing psychiatric disorders when addressed, but also to know the cumulative effect of these relevant risk indicators. From studies in the general population, it is known that the accumulation of risk factors, such as poor family functioning, high levels of parental stress and low family income, is exponentially related to the development of psychiatric disorders [37,38]. The severity of and impairment from psychiatric disorders is higher in families that experience negative influences in more than one area [32]. Children with two or more co-morbid psychiatric disorders and their families are also more likely to have other associated developmental, social, and educational needs [39]. Following this lead, young people with ID might be considered as a multi-risk group with complex and interrelated mental health needs over and above their intellectual disabilities. Therefore, the third aim of this was to determine the potential cumulative effect of reduction of all significant risk indicators in preventing psychiatric disorders in adolescents and young adults with ID.
To summarise, the present longitudinal study aimed, first, to identify risk indicators at ages 6 to 18 years that are predictive of psychiatric DSM-IV disorder 5-years later. Given the age and gender-sensitive development of specific psychiatric problems across adolescence and young adulthood, these two factors were considered moderators of the effects of potential risk indicators. Second, we aimed to contribute to developing effective preventive interventions by identifying the risk indicators associated with the largest potential health gain from preventive interventions. Third, we aimed to improve knowledge about the cumulative effect of risk indicators. This approach, seeking to identify high-risk groups of children with ID where preventive interventions are most likely to generate the largest health gains for the least effort, might yield important information relevant to the prevention of psychiatric symptoms in adolescents and young adults with ID.
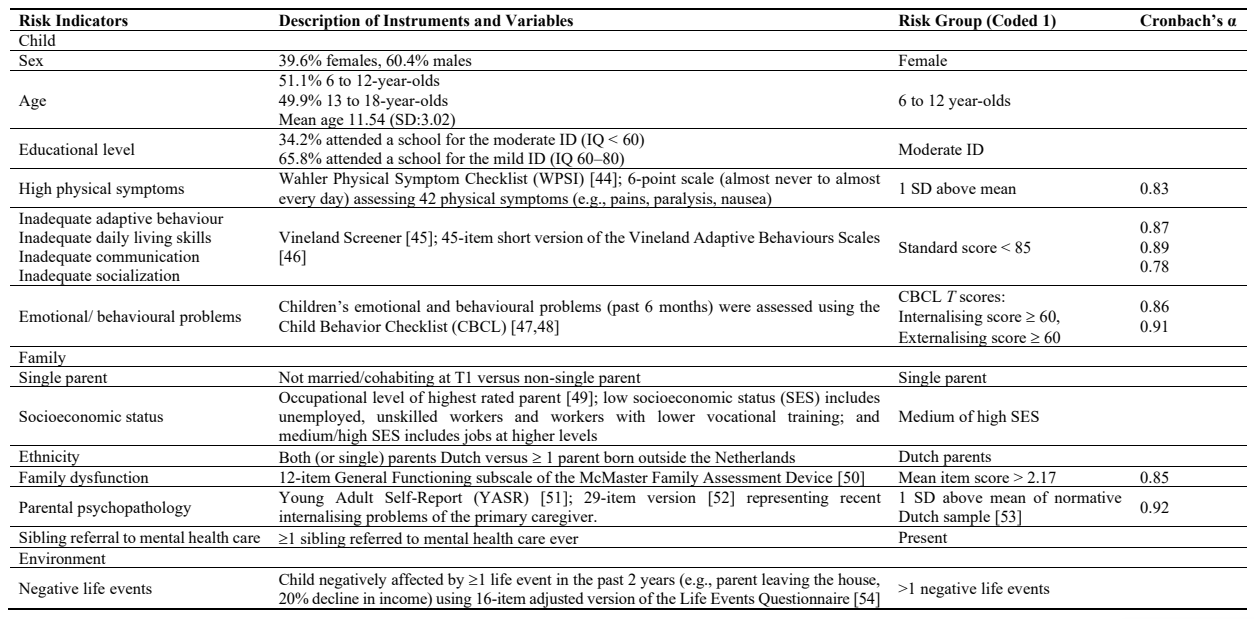
The present study used the first (indicated as Time 1, T1) and the third (Time 3, T3) parent assessments of a large random school-based study on psychopathology in Dutch children and adolescents aged 6–18 years at T1, with moderate to borderline ID. At T1 for 891 of 1396 children/adolescents eligible for this study, information for all addressed risk indicators was collected (response rate of T1 participants: 63.8%) (for more details on T1, see [4,29,40]). About 5 years after T1, 614 parents (T3 response rate: 68.8% of the participants at T1) were interviewed using the Diagnostic Interview Schedule for Children—Parent version (DISC-IV [41,42,43], after signing an informed consent form. For sample characteristics, see Table 1. We compared children/adolescents who participated at both times, excluding those who had incomplete data due to missing risk indicator information and/or missing DISC-IV interview data. No significant differences were found for age, sex, or deviant (i.e., above the borderline cut-off) CBCL total problem scores. However, children/adolescents who did not participate at both times more often came from families with low SES (versus medium or high SES, percentages: 69.9% vs. 47.7%, OR = 2.5, p < 0.001). They more often attended a school for children/adolescents with moderate ID (versus a school for children/adolescents with mild ID, percentages: 34.4% vs. 25.7%, OR = 1.5, p < 0.001) than children/adolescents who participated both at T1 and T3.
A description of putative risk indicators included in this study can be found in Table 1.
To assess the presence of any DSM-IV anxiety, mood, or disruptive disorder in the past year, the main caregiver was interviewed at T3 using the Dutch version of the DISC-IV [41,42,43]. The impairment criteria were not taken into account. The DISC-IV was administered by trained lay interviewers.
Univariate logistic regression analysis of each DSM-IV on each predictor was performed using SPSS version 12. Moderating effects of age and sex were tested separately by adding each variable and its interaction term with the main predictor variable to the model. If the model chi-square improved significantly, post hoc probing was performed to determine the significance and strength of the association between the main predictor variable and DSM-IV disorder within each moderator level. Next, linear probability models were tested using STATA [55] in three steps. In the first step, all predictor variables were entered into a backward stepping linear probability model. This model served to identify risk indicators with a significant contribution to the prediction of DSM-IV disorders. This step was carried out twice, first without including Internalising and Externalising, and second with Internalising and Externalising included as predictor variables. In the second step, the significant risk indicators from the previous step were used in parsimonious models to determine the potential relevance of the risk indicators in efforts to prevent DSM-IV disorders. The risk difference (RD) associated with each factor was obtained under a linear probability model and numbers to be treated (NNT) as a function of the RDs (NNT = 1/RD). In addition, incidence rate ratios (IRR) and attributable fractions (AF) were obtained under a Poisson regression model with the help of STATA’s Aflogit procedure [56]. In the third step, the possible cumulative effect of the risk indicators was investigated by calculating a risk index. This risk index represents the sum of the risk indicators that were found to have a significant OR. Since there were few children with 5 or more risks, the presence of 5, 6, 7 or 8 risks was combined into a new category “5 or more risks present” for Any DSM-IV, Any anxiety and Any disruptive disorder. Likewise, the category “3 or more” was created for Any mood disorder. In a next step, the risk indexes were used as predictors of DSM-IV disorders. The dose-response nature of the relationship between the risk index and the outcome was investigated using Kendall’s Tau.
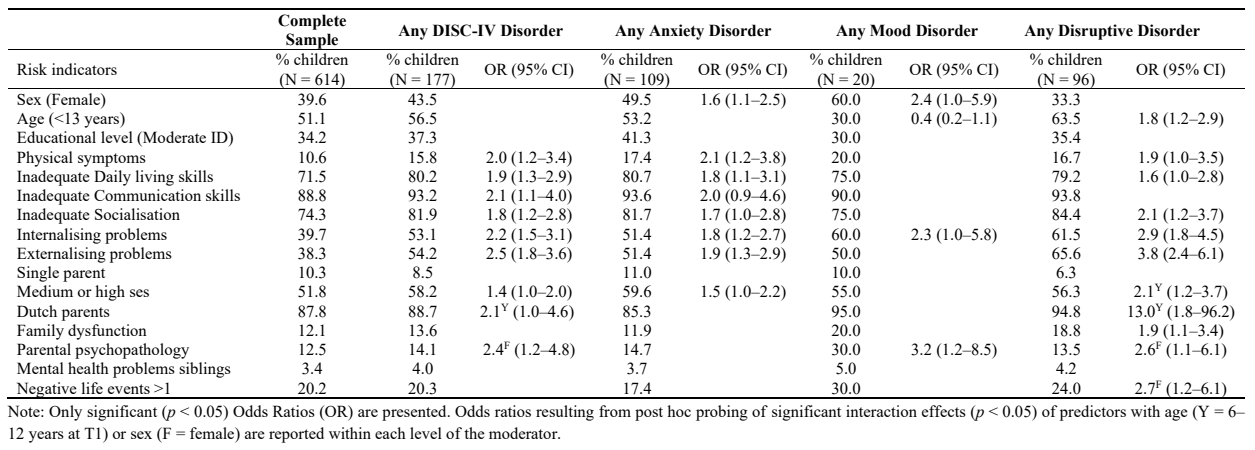
Table 2 shows the percentage of children exposed to each risk indicator, and the significant Odds Ratios within each level of the moderator variables age and sex whenever a significant interaction effect was present. All included factors except child educational level (mild vs moderate ID), single parenthood, and mental health problems in siblings were significantly related to one or more of the psychiatric disorder clusters. Only four significant interaction terms were found inconsistent across the four clusters.
After entering all significant risk indicators simultaneously in regression analyses several sets of indicators appeared as significant (p < 0.05) but independent contributors to the prediction of each DSM-IV disorder. For any DSM-IV disorder, the independent risk indicators appearing from these analyses were internalising, externalising, inadequate communication skills, and medium or high SES. For Any anxiety disorder, female sex, externalising problems, inadequate communication skills, and medium or high SES were the most relevant risk indicators. Any mood disorder was only significantly related to deviant levels of parental psychopathology. Finally, ages 6–12, internalising and externalising problems and having Dutch parents were the most relevant risk indicators for Any disruptive disorder.
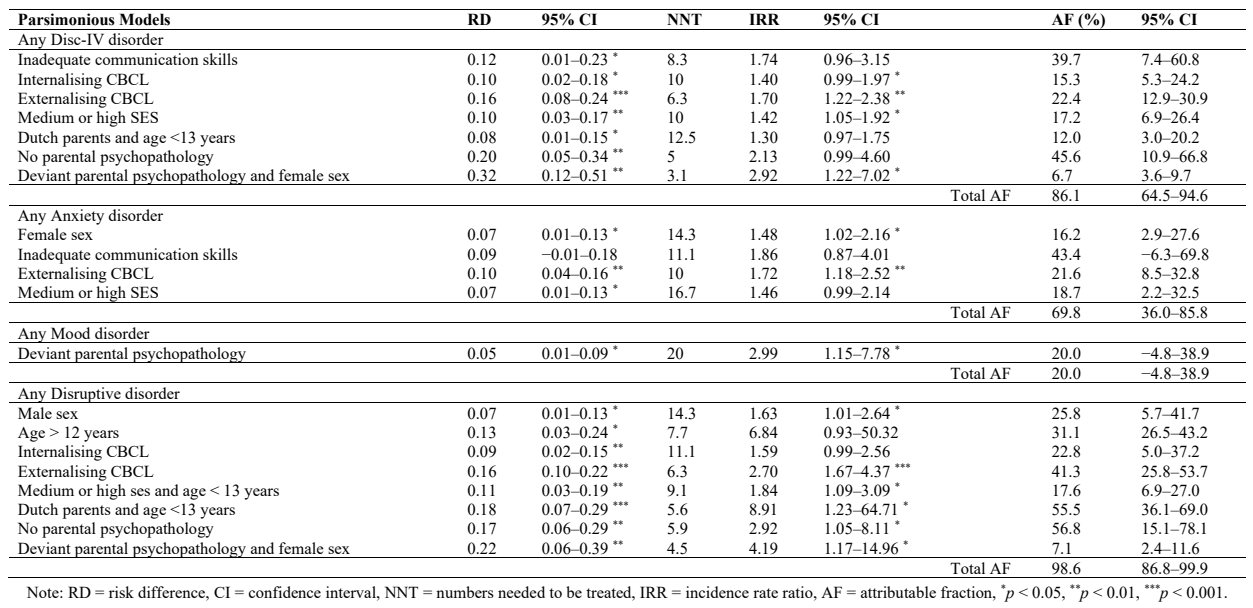
Table 3 presents the RDs, NNTs, IRRs and AFs of the parsimonious models described above. The risk indicators of the parsimonious models resulted in total AFs of 86.1%, 69.8%, 20.0%, and 98.6%, indicating the percentage of the cases of any DSM-IV, any anxiety, any mood and any disruptive disorder, respectively, that can be identified with these risk profiles.
Higher RD, IRR and AF and lower NNT indicate that a risk indicator is important for targeting preventive interventions. We use the first row of Table 3, corresponding to inadequate level communication skills, as an illustration to explain the findings reported in Table 3. The RD suggests a difference of 12% in the likelihood of having any DSM-IV disorder at T3 between children with inadequate and children with adequate communication skills at T1. The NNT of 8.3 indicates that 9 children would have to receive an intervention blocking the adverse effect of inadequate communication skills, in order to avoid one case with DSM-IV disorders, under the presumption that the intervention is completely successful in containing the adverse effect of this risk indicator. The IRR, which can be interpreted as an odds ratio, shows the increase in the probability of any DSM-IV disorder among the exposed group (children with inadequate communication skills) relative to the unexposed group (children with adequate communication skills). The AF value of 39.7% indicates that of all adolescents/young adults with any DSM-IV disorder at T3, 39.7% can be ascribed to inadequate communication skills at T1. In other words, if all children with inadequate communication skills at T1 had received an effective intervention to improve their communication skills, the prevalence of any DSM-IV disorder at T3 could have been reduced by 39.7%. The entries for the other risk indicators in Table 3 should be interpreted similarly.
The probability of having any DSM-IV disorder increased with the number of joint exposures to risk indicators; from 0.0% when having 0 risk indicators to 45.3% when having 5 or more risk indicators. When the significant risk indicators for any or a specific disorder were combined in a risk index and used as a single predictor of the outcome, the AFs attributable to this index were 80.2%, 84.0%, 44.6%, and 79.9% for any DSM-IV disorder, any anxiety disorder, any mood disorder, and any disruptive disorder, respectively. This indicates that approximately 80% of most DSM-IV disorders (except mood disorders) can be prevented when the negative effect of the combined risk indicators factors could be blocked. Accumulative exposures were significantly related to an increase in the risk for disorders (Kendall’s Tau = 0.25, 0.18, 0.06, and 0.17 for any DSM-IV disorder, any anxiety disorder, any mood disorder, and any disruptive disorder, respectively).
The main findings of this study are threefold. First, we found that not only childhood/adolescence levels of psychopathology but also child factors like inadequate adaptive functioning and family factors like parental psychopathology are important risk indicators for DSM-IV disorders in young people with ID who all after entering adolescence or young adulthood. Second, we found disorder specific Time 1 risk profiles, to which large proportions of the psychiatric problems in this sample identified 5 years later could be attributed. Third, similar to findings from the general population of children and adolescents, we found that the accumulation of risk factors increases the chances of developing a DSM-IV disorder, in this case, 5 years later. In the following section, we will discuss these findings in more detail.
The present study showed that when children have matured into adolescence or young adulthood, their levels of risk indicators from the child and family domain assessed at childhood or adolescence are still predictively associated with developed DSM-IV disorders. This extends the findings of Dekker and Koot [29], who looked into the 1-year predictive value of these child and family factors for the development of DSM-IV disorders in children and adolescents with ID using part of this same sample. In our study, independent and important risk indicators at the child level were internalising and externalising problems, inadequate communication skills, and at the family level and parental psychopathology. The previous study showed that the strongest 1-year predictive associations with DSM-IV disorders came from child social incompetence, inadequate daily living skills, health problems, emotional and behavioral problems, parental mental health problems and parent-reported negative life events. Apparently, next to child behavior problems, child/adolescent communication skills gain importance for predictive significance over this longer period. The risk indicators for psychopathology identified in this study are quite similar to those found for children and adolescents in the general population. In addition, inadequate daily living skills, specifically, inadequate communication skills, appeared as important predictors. It seems that with the increasing demands for independent functioning encountered during adolescence, these factors come to play a significant role in the development of mental health problems.
We found that parental psychopathology was the only significant risk indicator for mood disorders and that this factor alone can identify 20% of the cases of mood disorders in young people with ID. Apart from the important risk indicators included in this study, there might be other factors (e.g., genetic vulnerability and expressed emotion in the family [31,57] that are valuable risk indicators of psychiatric disorders too. It is quite likely that youths with ID are exposed more often to parental psychopathology than youths from the general population. We know that the likelihood of mental health problems is strongly elevated in people with ID and that a sizeable portion of parents of children with ID are affected by borderline to mild ID themselves.
Although, in accordance with what might be expected, females were more at risk for anxiety and mood disorders, and younger individuals more often had a disruptive disorder, very few moderation effects of gender and age were found. A significant finding was that females with ID were more affected by parental psychopathology and life events, specifically in the prediction of disruptive disorder.
A strong finding was that accumulation of risk factors was highly predictive of later psychiatric problems. The effect of the presence of multiple risks as opposed to a single risk in a child on the development of DSM-IV disorders had been found before in general population studies [58]. These studies showed that it is not the nature of risk factors but rather their number that is the best predictor of later outcome. More specifically, the more risk indicators present in the child and its family, the bigger the risk of psychopathology. In a study into risk indicators in children aged 2-3 years, it was shown that children who had a cumulative risk index of 3 or more risks were at a 50 times higher risk of problem behaviour [59]. Vervoort-Schel et al. [60] found that about 20% of the children with moderate and mild ID experienced 4 adverse childhood experiences or more. Many of their families faced multiple and complex problems. This pattern of cumulative incidence and effect was also found in adults with ID for the influence of life events on the development of psychopathology [32]. Some risk indicators (e.g., inadequate communication skills) are present in the majority (88.8%) of the sample. This makes the chance of having 2 or 3 risk indicators high, which might explain why the probability of disorder is especially high when the cumulative risk is 3 or more. The high percentage of multiple risk indicators in people with ID might partly explain the high prevalence of psychopathology compared to the general population, as found in many studies [1,5]. Screening for the cumulative risk status of children and adolescents with mild or moderate ID might enhance early detection of developing psychiatric problems at later ages.
The results of this study have potential meaning for the choice of targets for preventive interventions. For example, our findings on the influence of inadequate communication skills suggest that if all children with inadequate communication skills at T1 had received an effective intervention to improve their communication skills to an adequate level, the prevalence of any DSM-IV disorder at T3 could have been reduced by almost 40%. The attributable fractions (AF) for the several risk profiles established in this study (except for mood disorder) suggest almost full prevention options. However, only a few of the factors included in these profiles seem malleable and, therefore, the most likely options for targeting preventive interventions. These include child inadequate communication skills and both internalising and externalising problems next to parental psychopathology. That being said, the prediction models employed in this study are insufficient to imply interventions. Not only do the estimates in the parsimonious models fairly wide confidence intervals, but more importantly, no intervention is completely effective whatever actionable predictor is addressed. Randomized trials are indispensable to establishing true effectiveness.
The present study is not without limitations. First, the prevalence of mood disorders was low in our sample; therefore, we should interpret the results carefully. Future studies should focus on a larger sample of young people with ID and mood disorders in order to find out if sex and internalising problems in childhood should really not be included in a risk profile. Moreover, although not uncommon for this type of study, the non-response across waves of measurement in this study was rather large, and drop-out was not random, which may have influenced the reliability of our findings. Secondly, the diagnostic interview used in this study was designed for people without ID. It might be that people with ID express symptoms of disorders in a different manner than people without ID (e.g., expressing feelings of depression requires the ability to communicate on a high level). Also, some symptoms of depressive feelings, like having trouble focusing on (school)work, are inherent to the ID and might therefore, not be reported by their parents. Thirdly, predictions as obtained in this study might be influenced by unmeasured instability of the predictors across time up until the assessment of the outcome. For example, Erickson, Sroufe, and Egeland (1985) found a relationship between quality of attachment at 12 and 18 months and behavior problems in preschool, but much more so when attachment quality was stable.
This study shows that this group is vulnerable in multiple ways. In order to be able to prevent DSM-IV disorders in young people with ID, we need to focus on all the different areas in which these children experience negative influences and not on one single problem at the time. Parents, caregivers, teachers, and health care professionals should work together to monitor young children with ID. We can conclude three things: first, prevention should start early, when the first symptoms of internalising or externalising problems appear. Second, early training in communication skills for children with ID may prepare them better to face life’s challenges and provide more options for helping them reduce stress when needed. Third, parents need to be supported; when they experience mental health problems, they will have less resources to raise and support their children.
Future research is needed to replicate these findings and add risk indicators not currently included (especially in mood disorders). Also, future studies should focus on designing and evaluating prevention programs for young people with ID based on the risk profiles found in this study and in future studies.
We are very grateful for the contribution of all participants of this study, including the students of schools for special education, the parents, the teachers and supervisors, and the interviewers of adolescents/young adults and parents.
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Committee for Medical Ethics of the Erasmus MC-Sophia Children’s Hospital (Approval no. MEC 95.576).
This research was funded by grants from the Netherlands Health Research and Development Council (grant no. 28-2724), and the Sophia Foundation for Medical Research (grants no. 206 and no. 335).
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.