1. Introduction
Infants born with Hypoplastic Left Heart Syndrome (HLHS) and HLH variants are an extraordinarily complex, fragile group of patients with high rates of morbidity and mortality. They require stabilization in the early newborn period which, depending on their physiology, could require creation of an aorto-pulmonary shunt with or without aortic reconstruction or possible ductal stenting with pulmonary artery banding to complete their Stage 1 palliation(S1P). Following this surgery, they go through a very critical Interstage interval when their entire pulmonary blood flow depends on the patency of this surgical shunt. This is followed by Stage 2 palliation (S2P) that involves conversion to a systemic venous-pulmonary shunt (Glenn/Hemi-Fontan) at around 3–6 months of age.
The interstage period is critical for the survival of these infants [
1,
2,
3,
4]. Growth failure in this cohort has been shown to increase surgical complication rates, poor outcomes, and mortality [
1,
2,
3,
4].
In the year 2006, the National Pediatric Cardiology Quality Improvement Collaborative (NPC-QIC) was formed in the United States to improve outcomes in infants with HLHS [
5]. The collaborative sought to decrease interstage mortality, reduce growth failure, and reduce hospital readmissions due to major medical problems during the interstage period. The NPC-QIC has served to guide the Interstage Monitoring Programs (IMPs) throughout the country and now includes over 69 centers [
5,
6,
7,
8,
9,
10]. The IMP clinic at our institute has been participating in this collaborative since May 2009. Our aim was to evaluate the incidence of growth failure, and its potential modifiable risk factors in infants with HLHS followed by our IMP clinic over the last ten years.
2. Materials and Methods
This was a retrospective analysis of all the patients with HLH followed in our IMP clinic since its collaboration with NPC-QIC in 2009. The objective of our study was to study the somatic growth rate of infants with HLH followed by our IMP clinic from May 2009 to April 2019. We further aimed to identify the risk factors for growth failure in these infants during the interstage period (starting from discharge after S1P until admission for S2P). The secondary objective of the study was to compare the rate of transplant-free survival after S2P, prior to Fontan (stage 3 palliation) surgery in patients who achieved target interstage growth versus those who failed to do so.
Inclusion and Exclusion Criteria
The institute IRB committee reviewed and approved the study. All patients diagnosed with HLH physiology prenatally or postnatally were identified. These patients were transferred to our institute immediately after birth or after diagnosis was made (in the event of postnatal diagnosis) at the outside hospital. After their arrival to the hospital, a designated IMP member approached the parent or the legal guardian who obtained informed consent. These patients were then enrolled in the NPC-QIC Redcap database. An IMP team member met with the parents of enrolled patients after S1P and prior to hospital discharge and provided education regarding care of single ventricle infants at home. To meet discharge criteria, aside from being hemodynamically stable, the patient needed to demonstrate ability to tolerate some form of feeds and family needed to demonstrate ability to manage all feeds, medication, and medical devices with which their child is to be discharged home. These patients were sent home with an infant weighing scale and pulse oximeter. The digital infant scale provided is sensitive to weight changes ≤ 10 g. Following discharge, they were closely monitored by the IMP team until their admission for S2P. This monitoring included daily reporting and reviews of patients’ weights, heart rates, and oxygen saturation by the IMP team, clinic visits with clinician and a dietician every 1–2 weeks, and providing a 24-h phone line for parents to access the inter-stage team directly.
Enrolled patients who were discharged home following S1P in 2009 and had their S2P by April 2019 were included in the study. Patients who died, received heart transplant, or transferred care to another center prior to undergoing S2P were excluded. Patients who were never discharged after S1P until their S2P were also excluded as they did not follow with the IMP clinic.
Demographic data including birth weight, gender, gestational age, pre-natal diagnosis, presence of genetic or other major extracardiac anomaly, and type and time of surgery were collected. Data were collected regarding duration of hospital stay after the first surgery, any evidence or concern for necrotizing enterocolitis and type of feeding at discharge. The growth trends of these infants were studied during their interstage period.
The NPC QIC recommends a target growth rate of 20 to 30 g/day during the interstage period [
5,
6,
7]. Growth failure was defined as weight gain of ≤20 g/day during the interstage period. Weight gain for patients was assessed by comparing the first weight recorded in interstage period to the last weight recorded and divided over length of interstage period. Patients with growth failure were compared to those who achieved target growth rate using appropriate parametric and nonparametric tests of significance, using IBM SPSS (version 27.0). Continuous data was expressed in mean and standard error of mean (SEM) and analyzed using student-t test to compare the two groups. Categorical data were expressed in proportions and analyzed using Fisher’s Exact test, using a p value of 0.05 as significant. Multi-variate analysis was not performed due to the relatively small sample size.
3. Results
shows the flow diagram of the patients included in the study. From May 2009 to April 2019, 100 patients with HLHS were admitted to our hospital. Eighty-seven patients were discharged after S1P and enrolled in our IMP. Of these, 15 patients did not undergo S2P at our institute due to death, heart transplant, or transfer of care to another center.
. Flow diagram showing the incidence of growth failure amongst study subjects included in the interstage monitoring program (IMP). Note: About 26% of patients who underwent a Norwood/Sano experienced growth failure v. 21% who underwent a Norwood/BTT v. 72% of patients who underwent a Hybrid Palliation (<i>p</i> = 0.001).
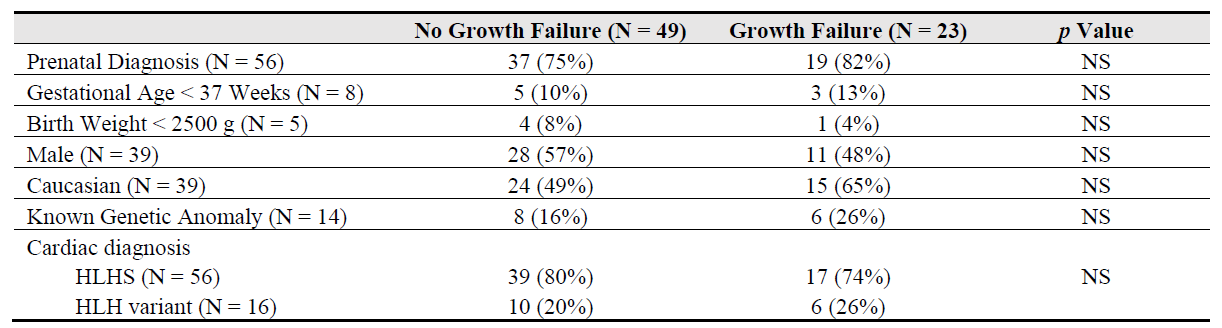
shows the baseline demographic characteristics of the study subjects. Majority of the patients (about 77%) had a prenatal diagnosis and only 5 (7%) were low birth weight. A known genetic anomaly was identified in about one-fifth (14, 20%) of patients. About 3/4th of the patients had classic hypoplastic left heart syndrome (with mitral and aortic atresia/stenosis) and no antegrade flow through the ascending aorta. Sixteen patients had HLH variant anatomy including unbalanced right ventricle dominant atrio-ventricular canal, double-outlet right ventricle with a hypoplastic left ventricle etc. Interestingly, the two groups did not have any significant baseline difference.
. Baseline characteristics of study subjects (n = 72). NS means not-significant.
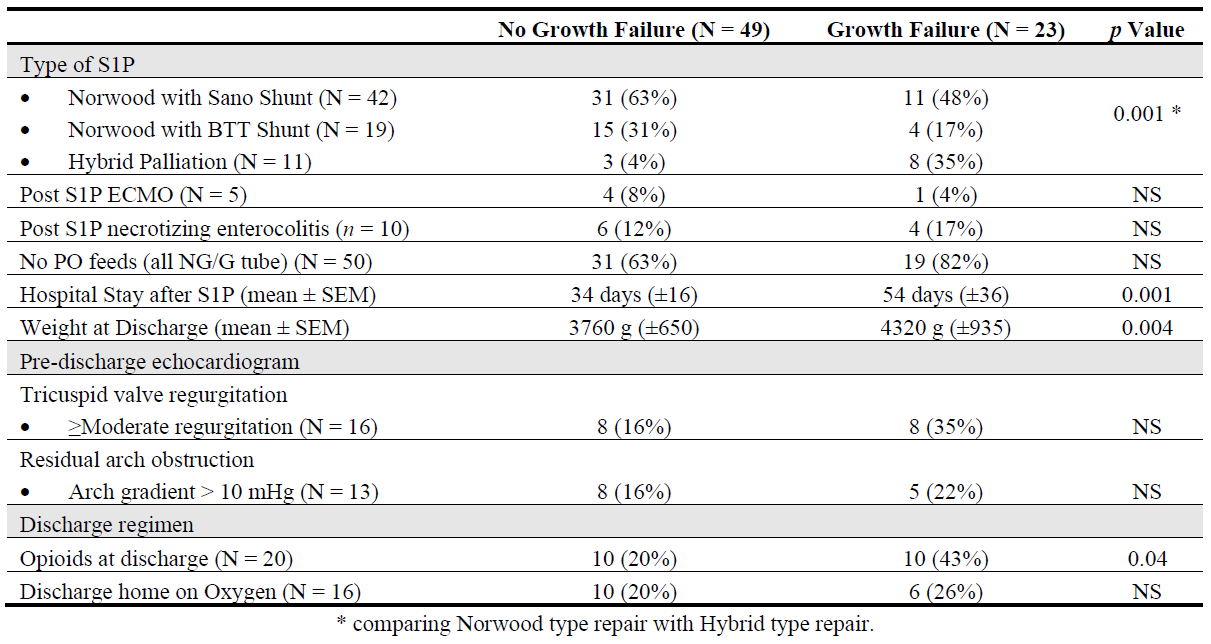
highlights the potential risk factors related to S1P which influenced the rate of somatic growth during interstage. Patients who suffered growth failure were significantly more likely to have undergone “Hybrid type of repair, consisting of pulmonary artery banding and patent ductus arteriosus stenting” as their initial procedure instead of Norwood type procedure (
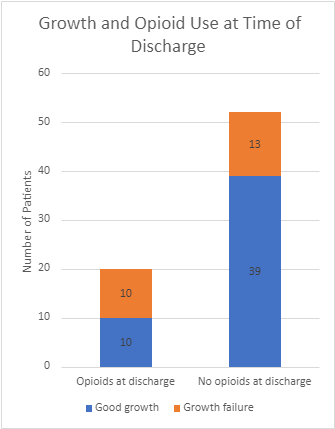
p = 0.001) as illustrated in . Pre-discharge echocardiogram showed that moderate or more tricuspid regurgitation was more common amongst patients with growth failure, however this was not statistically significant. Inability to wean off opioids prior to discharge was noted in 20/72 patients (28%). shows that when compared to those who were successfully weaned off opioids, those who were discharged home in opioids had a significantly higher rate of growth failure during interstage (
p = 0.04).
. Influence of Opioid use at time of discharge on growth failure. Image description: Growth failure was more common among the patients who were discharged home on opioids vs those who were not (50% vs 25%), <i>p</i> = 0.04.
. Pre and post-operative risk factors for growth failure following S1P. NS means not-significant.
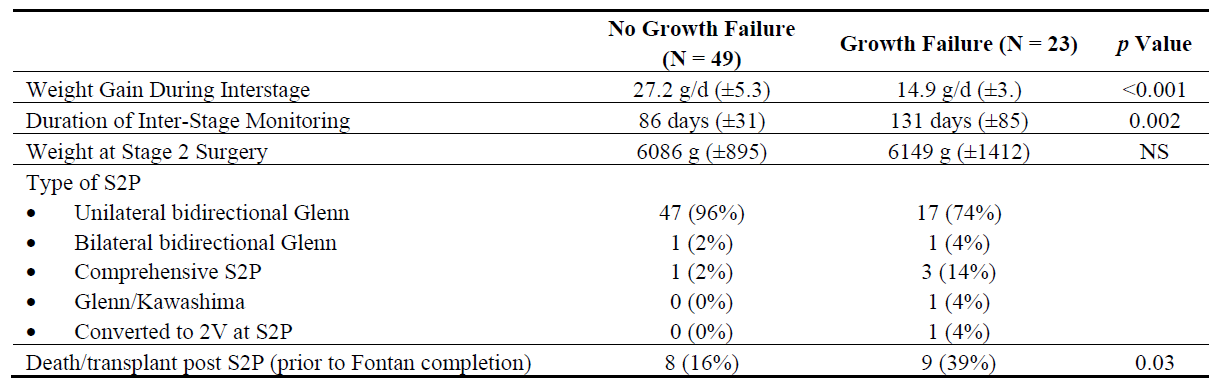
compares the clinical effects of growth failure on the study subjects. It is our center’s preference to perform the S2P between 4–6 months of age, and after achieving a weight gain of about 6 kg. It was noted that to achieve this target weight, patients with growth failure required a much longer duration of interstage monitoring (131 days vs 86 days). Most patients underwent unilateral, bidirectional Glenn procedure as their S2P. A total of 11 patients had undergone Hybrid repair in our study; and of these 7 patients underwent a separate PA de-banding and Norwood procedure, followed by Glenn surgery at a later stage. The remaining 4 patients underwent a comprehensive S2P consisting of a combined Norwood type arch repair and Glenn procedure. Majority of patients (84%) who achieved adequate interstage growth survived to S3P (Fontan) surgery, compared to only 61% who suffered from growth failure. A significantly larger proportion (39%) of patients with growth failure died or required a heart transplant following S2P (
p = 0.03).
. Clinical characteristics related to interstage growth in study subjects (N = 72). NS means not-significant.
4. Discussion
Infants born with functional single right ventricles (HLH) and variants are an extraordinarily complex, fragile group of patients with high rates of morbidity and mortality, especially during the interstage period when they are exposed to a shunt-dependent circulation [
8,
10]. Several interventions to improve survival have been studied, including home monitoring and early high calorie feeding plans. Investigators at Children’s Hospital of Wisconsin [
10] found that mortality was improved with close monitoring of weight at home, but despite intervention, weight gain plateaued at 4 months of age. Subsequent data from multicentric NPC-QIC collaborative found no relation between the frequency of interstage clinic visits with the rate of weight gain amongst these infants [
11]. These studies indicate that the growth rate during interstage is influenced from factors outside of the interstage period; and interventions done during interstage may not be sufficient to significantly reduce the extent of growth failure, and subsequent adverse clinical outcomes among these infants.
Indeed, our study found that the growth failure rates during interstage were largely influenced by pre-discharge factors. Neonates who had a longer duration of hospital stay after stage 1 surgery were at a significantly higher risk for growth failure. This likely indicates a more complicated post-operative course. These patients weighed more than their counterparts at discharge, which is an indirect indicator of a later age at discharge. Both the groups had similar weight when admitted for second stage surgery as the practice of our center is to perform S2P closer to a weight of 6 kg; however, the group with growth failure required significantly longer duration to achieve similar pre-Glenn weight (median interstage duration 131 days vs 86 days). Growth failure during interstage was thus associated with a delay in performing the second stage surgery and increased time in vulnerable shunt-dependent physiology. The rate of death or transplant after Glen surgery was significantly higher in patients with interstage growth failure and thus our study highlights the importance of interstage growth in overall outcomes in these patients.
The multi-centre single ventricle reconstruction (SVR) trial showed the impact of surgical approach during S1P to overall mortality during the first one year of life, with patients with Norwood-Sano repair showing a survival benefit over those who underwent a Norwood-BTT shunt approach [
12]. Our study was not powered to investigate the effect of Sano vs BTT shunt on interstage growth, but we found that the patients who underwent a Norwood-type repair were less likely to experience growth failure compared to patients who underwent a Hybrid Palliation. Hybrid palliation is typically offered to sicker newborns who are not considered good surgical candidates for primary Norwood surgery. Therefore, it is not surprising that this group of patients performed worse compared to their counterparts in achieving adequate growth.
It has been hypothesized that low birth weight may contribute to interstage patient’s poor nutritional status [
4]. Interestingly, in our study population, the incidence of low birth weight did not significantly differ in the two groups. Furthermore, we found no differences in mode of feeding between the two populations-whether patients were discharged home on exclusively nasogastric or gastrotomy tube feeds or tolerating some oral feeds. Given the nature of the chart review, we were unable to quantify if other qualitative feeding factors- such as persistent emesis- could have impacted their ability to gain weight.
The adverse outcomes of opioid dependence on single ventricle morbidity are well known. A recent multi-centre study from NPCQIC identified opioid dependence in these patients as one of the major factors predicting high mortality during interstage (NEONATE score) [
9]. Our study showed correlation between opioid prescription at discharge with likelihood of growth failure, which indirectly may impact interstage mortality. Our findings were internally shared with our team, and efforts to reduce opioid use in during their postoperative stay are being implemented. Future research may be targeted to study the effect of these interventions on overall reducing interstage growth failure and interstage mortality.
Ahmed et al. analyzed the multi-centric NPCQIC database and found some anatomical features associated with poor second stage outcomes [
9]. One of the primary risk factors contributing to increased interstage mortality was more than moderate degree of systemic tricuspid valve regurgitation. Significant tricuspid regurgitation was also more common in our patients with growth failure, however this difference did not reach statistical significance, likely due to our relatively smaller sample size.
Our study has several limitations. While our study indicates that HLHS infants with interstage growth failure have a lower S2P transplant-free survival, this could not be established as an independent risk factor; since the relative smaller study sample did not allow a thorough multi-variate analysis, exploring several other predictors of post-Glenn mortality including pre-Glenn hemodynamics, post-operative ECMO, incidence of necrotizing enterocolitis etc. [
8,
9,
10]. Given the retrospective nature of the study, complete socio-demographic information of the patients was not available, and we were unable to assess if certain social determinants of health- such as economic stability or living environment- had an impact on this population. The study results may also not be generalizable to other centers. However, conducting the study at a single institution may avoid the potential bias that may occur from variability in surgical techniques, and postoperative care amongst institutions.
In conclusion, interstage growth failure is common in HLHS patients, despite active intervention through an IMP program. These patients appear to have significantly worse transplant-free survival rates. Pre-interstage risk factors including use of opioids may need to be addressed to assist adequate somatic growth during interstage.
Acknowledgments
The authors would like to acknowledge NP Courtney Howell and Amy Svenson, MD for their contribution to the initial data collection.
Author Contributions
K.B.: Data analysis, Revision and review of the manuscript; J.N.G.: Revision and review of the final draft of the manuscript; D.P.B.: Conceptualization, development of the study design and methods, data analysis, preparation of the initial draft and final revision.
Ethics Statement
The institutional IRB approved the study.
Informed Consent Statement
Informed consent was obtained from the parents of all study subjects at the time of enrollment.
Funding
None.
Declaration of Competing Interest
The authors have no financial disclosures.
References
1.
Kelleher DK, Laussen P, Teixeira-Pinto A, Duggan C. Growth and correlates of nutritional status among infants with hypoplastic left heart syndrome (HLHS) after stage 1 Norwood procedure.
Nutrition 2006,
22, 237–244.
[Google Scholar]
2.
Vogt KN, Manlhiot C, Van Arsdell G, Russell JL, Mital S, McCrindle BW. Somatic growth in children with single ventricle physiology impact of physiologic state.
J. Am. Coll. Cardiol. 2007,
50, 1876–1883. doi:10.1016/j.jacc.2007.07.050.
[Google Scholar]
3.
Hehir DA, Cooper DS, Walters EM, Ghanayem NS. Feeding, growth, nutrition, and optimal interstage surveillance for infants with hypoplastic left heart syndrome.
Cardiol. Young 2011,
21 (Suppl 2), 59–64. doi:10.1017/S1047951111001600.
[Google Scholar]
4.
Golbus JR, Wojcik BM, Charpie JR, Hirsch JC. Feeding complications in hypoplastic left heart syndrome after the Norwood procedure: A systematic review of the literature.
Pediatr. Cardiol. 2011,
32, 539–552.
[Google Scholar]
5.
Clauss SB, Anderson JB, Lannon C, Lihn S, Beekman RH, Kugler JD, et al. Quality improvement through collaboration: The National Pediatric Quality Improvement Collaborative initiative.
Curr. Opin. Pediatr. 2015,
27, 555–562. doi:10.1097/MOP.0000000000000263.
[Google Scholar]
6.
Slicker J, Hehir DA, Horsley M, Monczka J, Stern KW, Roman B, et al. Nutrition algorithms for infants with hypoplastic left heart syndrome; birth through the first interstage period. Congenit.
Heart Dis. 2013,
8, 89–102. doi:10.1111/j.1747-0803.2012.00705.x.
[Google Scholar]
7.
Rudd NA, Ghanayem NS, Hill GD, Lambert LM, Mussatto KA, Nieves JA, et al. Interstage Home Monitoring for Infants With Single Ventricle Heart Disease: Education and Management: A Scientific Statement From the American Heart Association.
J. Am. Heart Assoc. 2020,
9, e014548. doi:10.1161/JAHA.119.014548.
[Google Scholar]
8.
Brown DW, Mangeot C, Anderson JB, Peterson LE, King EC, Lihn SL, et al. Digoxin Use Is Associated with Reduced Interstage Mortality in Patients with No History of Arrhythmia After Stage I Palliation for Single Ventricle Heart Disease.
J. Am. Heart Assoc. 2016,
5, e002376. doi:10.1161/JAHA.115.002376.
[Google Scholar]
9.
Ahmed H, Anderson JB, Bates KE, Fleishman CE, Natarajan S, Ghanayem NS, et al. Development of a validated risk score for interstage death or transplant after stage I palliation for single-ventricle heart disease.
J. Thorac. Cardiovasc. Surg. 2020,
160, 1021–1030. doi:10.1016/j.jtcvs.2019.11.001.
[Google Scholar]
10.
Ghanayem NS, Hoffman GM, Mussatto KA, Cava JR, Frommelt PC, Rudd NA, et al. Home surveillance program prevents interstage mortality after the Norwood procedure.
J. Thorac. Cardiovasc. Surg. 2003,
126, 1367–1377. doi:10.1016/s0022-5223(03)00071-0.
[Google Scholar]
11.
Hurst DM, Oster ME, Smith S, Clabby ML. Is Clinic Visit Frequency Associated with Weight Gain During the Interstage Period? A Report from the Joint Council on Congenital Heart Disease National Pediatric Cardiology Quality Improvement Collaborative (JCCHD-NPCQIC).
Pediatr. Cardiol. 2015,
36, 1382–1385. doi:10.1007/s00246-015-1169-6.
[Google Scholar]
12.
Jaquiss RDB. The Single Ventricle Reconstruction trial: The gift that keeps on giving.
J. Thorac. Cardiovasc. Surg. 2016,
151, 676–677. doi:10.1016/j.jtcvs.2015.09.095.
[Google Scholar]