1. Introduction
Type 2 diabetes (T2D) is one of major non-communicable diseases (mNCDs) that requires lifelong treatments and management of high glycemic level. More than 400 million adults worldwide suffer from diabetes [
1]. Obesity, physical inactivity, and unhealthy diet are major risk factors in adults diabetes [
2], and racial & ethnic groups, maternal obesity have also led to a relative increase in T2D. In fact, the incidences of both type 1 and T2D increase significantly, particularly among minority racial and ethnic groups [
3]. Although mortality and fatal outcomes declined in individuals with T2D in some developed countries [
4], for example, in Sweden from 1998 through 2014, it’s still a big challenge and a heavy burden in developing countries.
Since high-quality care for individuals with T2D could decrease unnecessary emergency visits [
5], for example, urine glucose screening within community and schools may help to detect early asymptomatic T2D [
6], and individuals with T2D need to exercise more often (at least meeting physical activity guidelines) for reduction of mortality [
7]. However, considerable proportion of T2D patients in some Asian countries and regions, for example, South Korea, were not adequately managed and lack of high-quality care due to no reliable comprehensive program [
8]. In addition, a large-scale international study showed that subjects with T2D frequently have depression and psychological and psychiatric problems [
9]. Thus, there is arising evidence for better management of T2D, since it is an independent predictor of revascularization and long-term mortality [
10]. Based on these features of T2D (high prevalence, high risk for adverse clinical outcomes, and high burden of public health) as well as lack of a high quality program for management of T2D, we wrote this review and aim to conduct a novel comprehensive program combining optimal medical treatment (OMT) with lifestyle modification for T2D.
2. Current Status and Main Treatment of T2D
T2D is one of the most prevalent diseases and one of the leading causes of morbidity and mortality worldwide. Currently, over 10.5% of the adult population has been diagnosed with T2D, and almost 12% of total health expenditure is spent exclusively on T2D management globally. And there is increasing incidence of T2D among youth since the incidence of overweight and obesity among children has increased dramatically in recent decades. However, most youth with T2D do not achieve optimal glycemic control, and are at high risk for later cardiometabolic health complications, which include microvascular complications (nephropathy, neuropathy, and retinopathy) and macrovascular complications, such as acute myocardial infarction (AMI), chronic heart failure (CHF), and strokes.
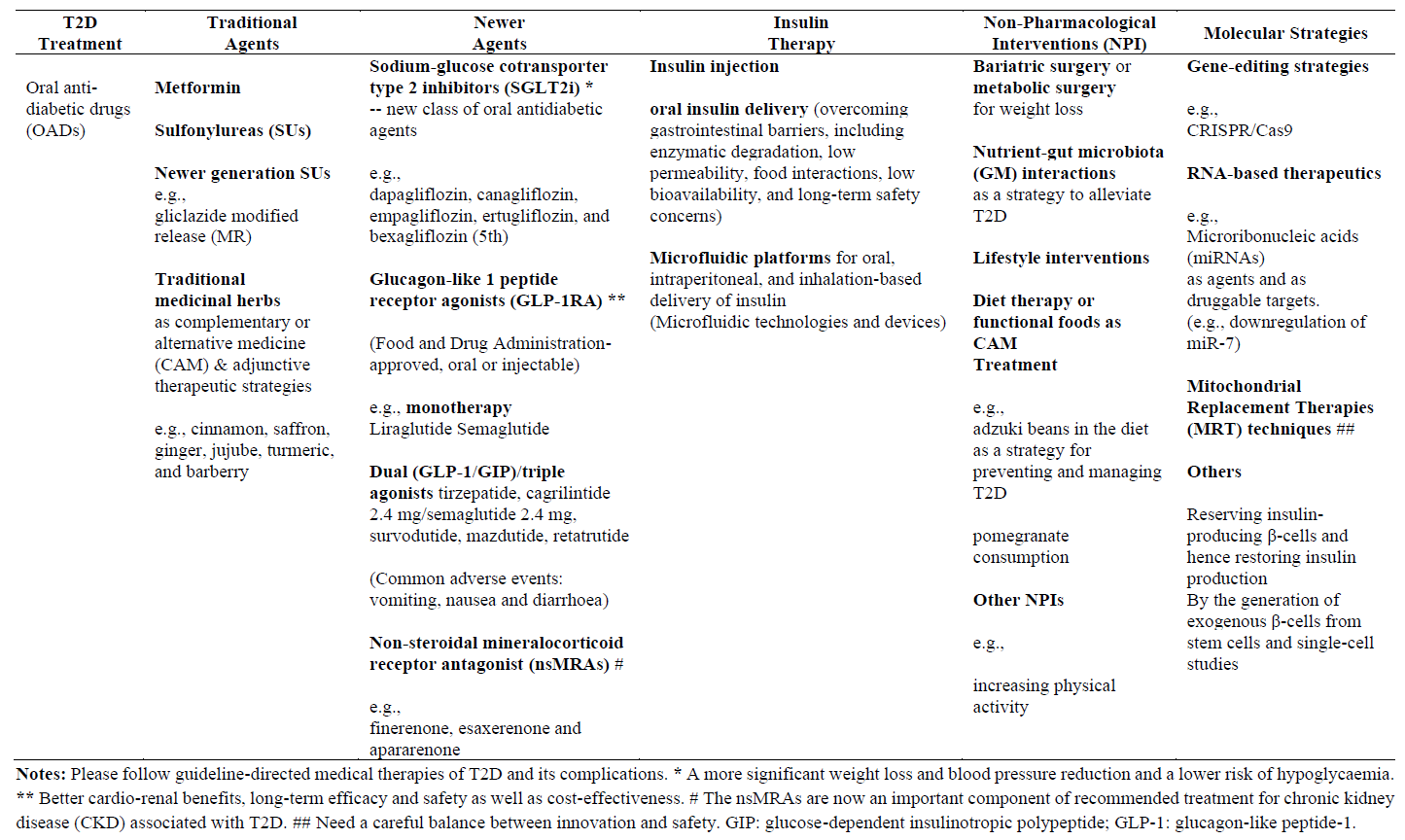
Currently, treatment of T2D focuses on glucose-lowering medication and non-pharmacological treatment. () The former includes oral hypoglycemic agents, insulin pump or injection therapy; The later includes surgical treatment, for example, bariatric surgery for markedly obese individuals with T2D, and modification of unhealthy lifestyle. Newer anti-diabetic drugs such as the sodium-glucose cotransporter 2 (SGLT2) inhibitors (SGLT-2i) and the glucagon-like peptide-1 receptor (GLP-1 R) agonists (GLP-1 RA) can reduce the risk of both microvascular complications and macrovascular disease in patients with T2D. However, most patients with T2D have not achieved optimal glycemic control with mono-therapies. Moreover, some treatments may have side-effects [
11]. Although current guidelines for T2D are suitable for clinical doctors to use, it isn’t for individuals’ self-management of T2D. Of course, there is still a need for self-control of glucose levels in a new era of personnel medicine.
Since current main treatment of T2D remains a challenging issue, and therapeutic goals are often not achieved. Herein, we proposed the iRT-ABCDEFG program combining OMT with lifestyle modification as a novel comprehensive strategy for better T2D management.
. Current main treatment of T2D.
3. An Updated Standardized Comprehensive Program
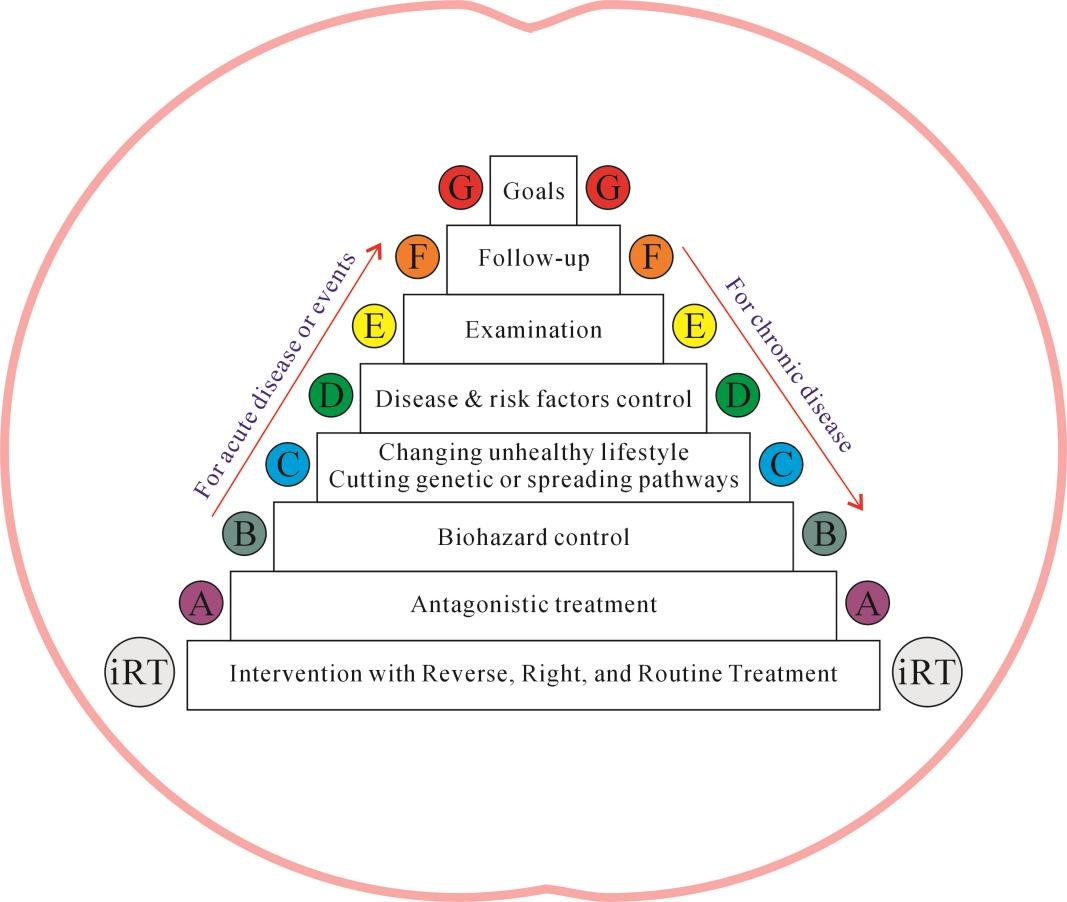
How can an individual control and prevent T2D with a simple and effective method? We strongly recommend an updated classical standardized comprehensive iRT-ABCDEFG program () for clinical professional management and family health care of T2D. Here, G means goals; F means follow-up; E means examination; D means disease & risk factors control; C means changing unhealthy “environment-sleep-emotion-exercise-diet” intervention [E(e)SEEDi] lifestyle & Chinese medicine or control the source of infection & cutting genetic or spreading pathways during the COVID-19 pandemic; B means biohazard control; And A means antagonistic treatment, such as optimal anti-diabetic agents, which include traditional agents (for example, metformin and others), and novel chemical agents, such as [GLP-1 RA, SGLT-2i, the ultralong-acting, once-daily basal insulin, and others].
. The iRT-ABCDEFG program for managing type-2 diabetes (T2D).
According to this figure, it’s easy to understand that this comprehensive program is very helpful to control and prevent T2D and reach several pivotal goals after consistently practice, which include less major adverse cardiocerebrovascular events (MACCE) and diabetic complications, less medical costs, longer life expectancy, lower morbidity and mortality, and higher quality of life, due to early diagnosis, OMT, and healthy E(e)SEEDi lifestyle for overall prevention. Herein, this iRT-ABCDEFG program is worthy of recommending for clinical professional management and health care of T2D due to better cost-effectiveness. However, it needs to confirm by long-term follow-up and clinical trials. In fact, it is suitable for not only acute diseases or events, such as acute myocardial infarction (AMI), stroke, and COVID-19 infection, but also chronic diseases, such as C-type hypertension (CtH), chronic heart failure (CHF), chronic kidney disease (CKD), neurodegenarative diseases (dementia or Alzheimer’s disease and Parkinson’s disease), and cancer as well as the cardiovascular, diabetes, and cancer (CDC) strips.
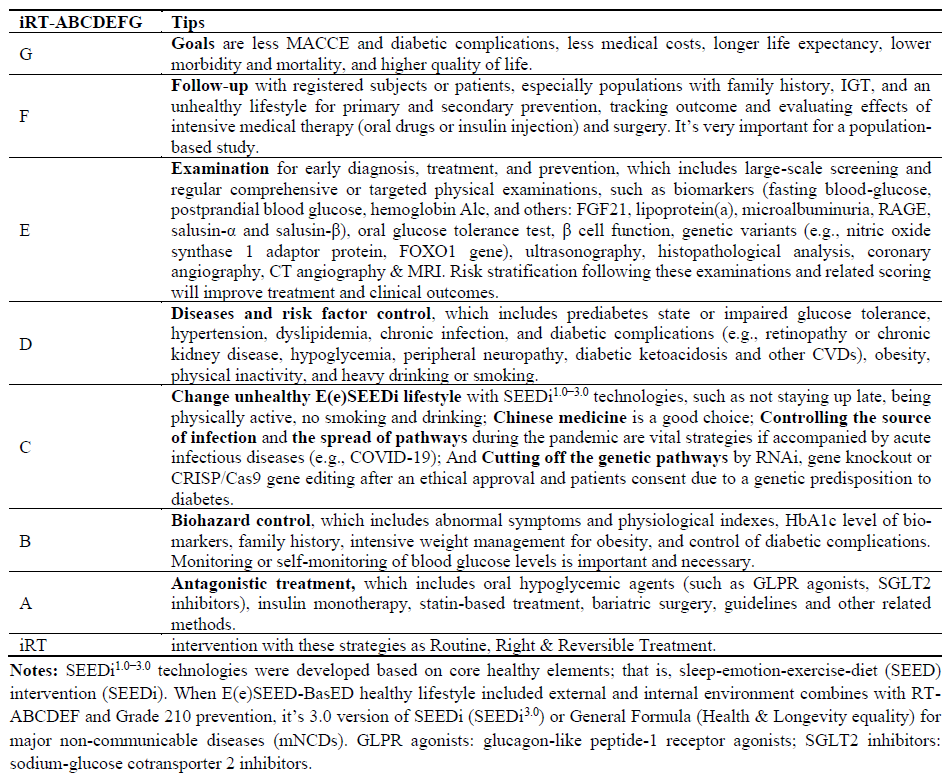
As a novel strategy for Intervention of diabetes, this program can be used as a Reverse, Right, and Routine Treatment in clinical practice. The detailed tips are as follows ().
This iRT-ABCDEFG program is very suitable for not only control of risk factors and cardiovascular disease (CVD), e.g., hypertension [
12], AMI [
13], CHF [
14], and arrhythmogenic right ventricular cardiomyopathy [
15] as well as cancer [
16] and major virus-communicable diseases [
17], but also T2D. Firstly, good goals help to work better. Moreover, as an updated classical, individualized, and concise “guideline”, if treated as “a law” in clinical practice, the vital goals which include less MACCE and diabetic complications, less medical costs, longer life expectancy, lower morbidity and mortality, and higher quality of life, will be realized by consistently practicing this iRT-ABCDEFG program due to early diagnosis, OMT, and overall prevention by healthy E(e)SEEDi lifestyle.
On the one hand, follow-up of both doctors with patients and patients with doctors will improve outcomes. For example, follow-up found that intensive glucose control reduces MACCE [
18], but bariatric surgery plus intensive medical therapy is more effective for control hyperglycemia than intensive medical therapy alone [
19]. Individuals’ comprehensive or targeted examinations or population-based large-scale screening (e.g., urinary glucose screening) will help the early diagnosis of both symptomatic and asymptomatic T2D [
6,
20]. For example, there are only 10% undiagnosed cases of diabetes in the United States due to large-scale screening, and diagnoses by the criteria of elevated levels of fasting glucose (≥7.0 mmol/L) and hemoglobin A1c (HbA1c, ≥6.5%) [
21].
Since postpartum follow-up and screening of oral glucose tolerance test (OGTT) during the delivery hospitalization is helpful to control maternal T2D, follow-up of women after delivery and scheduled screening for preventing T2D is very important for against this public health issue. Whatever, early examination and screening will help the management of T2D and decreasing its complications. Some serum biomarkers are helpful to determine its severity and complications, such as fibroblast growth factor 21 (FGF21) [
22], the receptor for advanced glycation end products (RAGE) [
23], and salusin-α and salusin-β levels [
24]. In addition, albuminuria level is also associated with higher risk of MACCE (AMI, stroke) in patients with T2D [
25].
On the other hand, this program helps to control T2D-related complications and major risk factors by cutting genetic pathways and changing unhealthy lifestyles, which can also decrease diabetic gene mutation. Studies have already shown that intensive lifestyle intervention in patients with T2D is beneficial to control individuals’ glycemic levels [
26], e.g., intensive body weight management [
2]. Moreover, healthy lifestyle included five core elements—“environment-sleep-emotion-exercise-diet” intervention [E(e)SEEDi] [
27,
28] may achieve better goals in control and prevention of T2D () [
29,
30,
31,
32,
33,
34,
35,
36,
37,
38,
39,
40,
41,
42,
43].
. The iRT-ABCDEFG program as a standardized comprehensive program for T2D.
As we already known, CVD and T2D are more common in some populations (such as taxi drivers) due to unhealthy lifestyle [
44]. However, healthy lifestyle is associated with a lower risk of CVD incidence and mortality among adults with T2D [
45], it plays a key role in risk factor management for primary prevention of CVD [
46]. In fact, lifestyle modification can reduce risk factors in both CVD and T2D [
47]. However, current lifestyle modification is still low among US adults with chronic conditions [
48]. Therefore, healthy E(e)SEEDi lifestyle should be recommended to all individuals in the globe.
Previous studies showed that exercises were associated with significantly lower HbA1c and fasting blood glucose [
49], and plant-based diets which include legumes, whole grains, vegetables, fruits, nuts, and seeds, not only reduce the risk of T2D but also help to prevent T2D [
50]. However, there are no significant difference in MACCE from n-3 fatty acid supplementation among T2D patients without CVD [
51], Vitamin D
3 supplementation did not result in a significantly lower risk of T2D [
52]. Without a doubt, individualized biohazard control and antagonistic treatment are necessary according to “5P” medical model [
53], because T2D can easily result in injury of organs and a series of complications without long-term optimal glycemic control, for example, erectile dysfunction, lipoprotein (a) and microalbuminuria are predictors of vascular complications [
54,
55,
56]. The EUCLID Trial showed that every 1% increase in HbA
1c was associated with a 14.2% increased relative risk for MACCE in patients with diabetes and peripheral artery disease [
57]. There are less costs and better quality of life among patients with individualized glycemic control than uniform intensive control (HbA1c level < 7%) [
58].
On antidiabetic medical treatment, clinical studies already showed that the GLPR agonists, semaglutide [
59] and liraglutide [
60,
61,
62] the SGLT2 inhibitors [
63], canagliflozin [
64,
65] and empagliflozin [
66,
67,
68], and an ultralong-acting, once-daily basal insulin degludec [
69], are not only helpful to glycemic control but also reduce MACCE including cardiovascular death or hospitalization for heart failure (HHH) in subjects with T2D and/or slower progression of diabetic chronic kidney disease (CKD). Since both were not associated with high rates of venous thromboembolism [
70], the SGLT2 inhibitors and the GLPR agonists had already been recommended by the 2019 guidelines of American Diabetes Association (ADA) [
71]. It can be said that 2 new classes of antihyperglycemic agents [
72], the GLPR agonists and the SGLT2 inhibitors, have indeed led to a paradigm shift of T2D treatment. However, a study found that, a selective SGLT2 inhibitor dapagliflozin [
73], not result in a higher or lower rate of MACCE, but in a lower rate of cardiovascular death or HHH.
In addition, the nonsteroidal, selective mineralocorticoid receptor antagonist (MRA) finerenone can reduce the risk of new-onset atrial fibrillation or flutter (AF/AFL) in patients with T2D and CKD [
74]. Of course, there is still improper use of aspirin for primary and secondary prevention of CVD in T2D [
75]. According to its cost and safety profile, metformin should be the first line drug therapy for patients with newly diagnosed T2D [
76]. Due to cardiovascular benefit and lower achieved LDL-C levels associated with lower risk of MACCE [
77], statin therapy should be recommended for primary prevention in the elderly with or without T2D [
78]. In fact, it is also easy to understand the treatment of T2D and its complications from other systematic reviews, including relatively complete existing drugs, therapeutic effects, adverse events, and other aspects. Therefore, we will not list and summarize here.
4. Advantages of the iRT-ABCDEFG Program
Since T2D is as dangerous as coronary heart disease and associates with higher MACCE, which include cardiovascular and non-cardiovascular hospitalizations, AMI, CHF, ischemic stroke/TIA recurrence, and death [
79], abnormal glycemic levels link to high mortality and morbidity. For example, on the one hand, maternal T2D highly links to arterial stiffness, cardiac hypertrophy, and congenital heart defects; On the other hand, there is increasing T2D in offspring in late adult life due to maternal gestational hypertension. Thus, we think that there are obvious advantages of this iRT-ABCDEFG for T2D, which will help to realize the European Society of Cardiology’s ambitious mission “to reduce the burden of CVD” in countries worldwide [
80].
Most cases of new onset T1D in China occurred among adults [
81], this iRT-ABCDEFG program is suitable for not only T2D but also T1D because it can help to decrease and delay onset of T1D by healthy E(e)SEEDi lifestyle and cutting a genetic pathway in the early stage of one’s lifetime due to control of maternal risks. Thus, this iRT-ABCDEFG program is worthy of conducting in the globe. In addition, since T2D is surprisingly closely linked to AMI, CHF, and stroke, diabetic chronic kidney disease (CKD), maximum effort must be made to control the prevalence of T2D so as to halt CVD and its costs increasing. Since policy initiatives can help controlling increases in health care spending [
82], it’s time for not only
Health in All Policies but also
Health in All Laws [
16,
83].
With the further studies on mechanisms and the continuing development of new drugs and novel technologies for T2D, more precise and effective management or self-management of T2D with this iRT-ABCDEFG program is possible due to the role of structure-editing on unhealthy lifestyle [
84], and long-term trends in mortality and the incidence of MACCE will also decline. For example, a clinical trial confirmed that oral insulin 338 can safely improve glycaemic control in insulin-naive patients with T2D, although it isn’t in place of subcutaneous insulin glargine yet due to being not commercially viable at current stage [
85].
In short, since some cardiovascular metabolic factors of T2D, such as obesity, physical inactivity, obstructive sleep apnea (OSA), hypertension, and other modifiable unhealthy E(e)SEEDi lifestyle-related factors, may induce MACCE (AF, AMI, CHF, Stroke) and reduce health span and life span [
86,
87], control and prevention of these risk factors according to this iRT-ABCDEFG program will get more clinical benefit and improve cardiovascular outcomes. The SGLT2 inhibitors and GLP-1 receptor agonists, the newer classes of antihyperglycemic agents with the cardiorenal protective effects [
88], will add distinctly clinical benefit. The MRA finerenone also reduces the composite kidney and cardiovascular outcomes [
89].
5. Future Perspective
It can be easily found that this comprehensive program will help to translate new technologies and research into clinical practice and reverse T2D due to strengthening prevention and management or self-management as well as personalized services. It will meet not only Healthy China 2030 Plan but also updated the National Health Service (NHS) Long Term Plan in the UK [
90]. In short, this program can help to achieve global health goals.
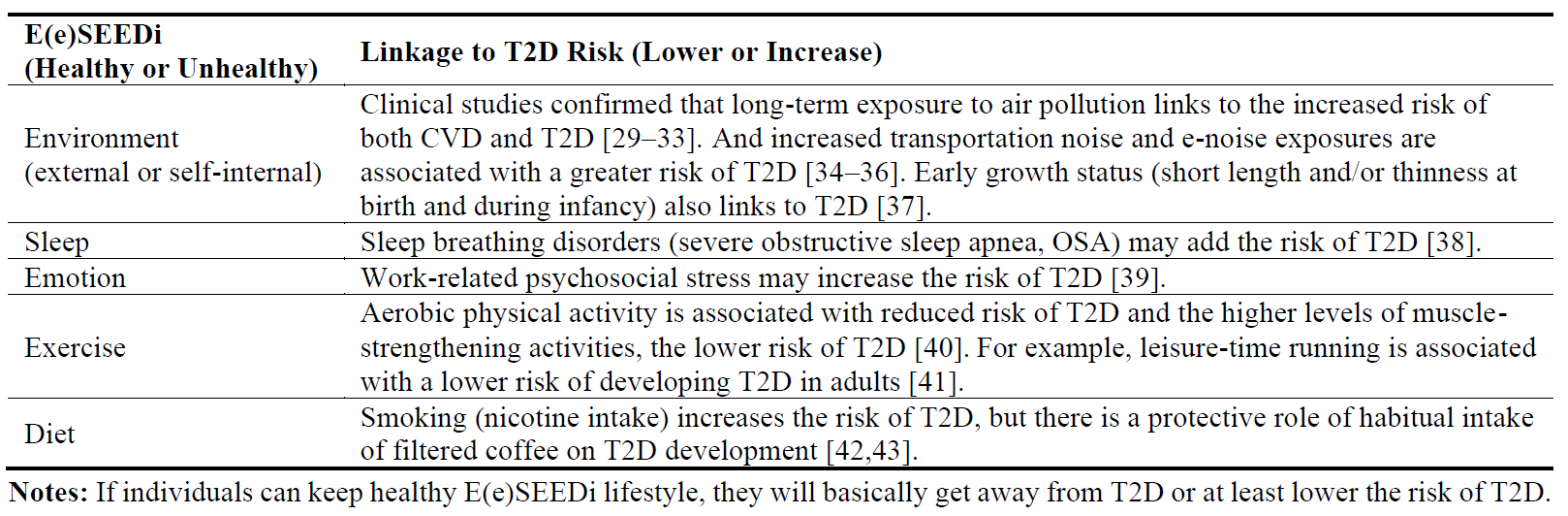
In fact, this program has already been used for CVD and cancer in daily clinical practice, but there are more detailed recommendations for on changing an unhealthy lifestyle to manage T2D (). If there was a national registered centre for T2D, similar to those for major communicable diseases like SARS and COVID-19 [
17,
91], more satisfactory results could be achieved through reliable national clinical trials using this innovative comprehensive program. This program combines anti-diabetic agents, insulin use, metabolic surgery, mental health screenings, and the healthy E(e)SEEDi lifestyle [
27,
92,
93], which includes a plant-based diet. This approach could lead to better control of population-level HbA1c and cardiovascular risk among individuals with T2D.
. The effects of healthy or unhealthy E(e)SEEDi lifestyle on T2D: Evidences from PubMed literature.
With a better understanding in the pathophysiological mechanisms at the molecular level and the discovery of new targets for metabolism [
94,
95], the implications for existing guidelines and therapeutic options, as well combination with this iRT-ABCDEFG program and effective lifestyle interventions for T2D, for example, a precision dietary management and scientific dietary recommendations with respect to carbohydrate, fat and dietary fibre, and increases in physical activity and fitness, calorie restriction and weight loss [
96,
97], these individuals will improve greatly glycaemic control and better prevent its complications [
98], such as CVD and neurodegenarative diseases (Alzheimer’s disease and Parkinson’s disease) [
99]. In addition, the prevalence of both depression and thyroid abnormalities is high among individuals with T2D [
100,
101]. and coronary plaques [
102], abnormal gene expression and serum biomarker levels in these patients mean higher risk and adverse clinical outcomes [
103,
104,
105], hence, we should control and prevent these risk factors so as to reduce cardiovascular mortality.
Theoretically, this iRT-ABCDEFG program is more plausible for better management and self-management of T2D due to truly individualized glycaemic goals. Early detection of ischemic heart disease and unrecognized CHF is beneficial for individuals with T2D. Treatment with statins and SGLT2 inhibitors can safely improve lipid levels and endothelial function, ultimately lowering the risk of MACCE [
106]. Additionally, a biomarker score can be used to stratify the risk of CHF in individuals with T2D and pre-diabetes [
107]. Healthy E(e)SEEDi lifestyle may help to reduce these risks and improve clinical outcomes [
108]. In addition, clinical trials already confirmed benefits of selective nonsteroidal MRA eplerenone [
109] and finerenone [
110] in CHF prevention and cardiovascular outcomes improvement. Obviously, a combination of these strategies in this novel comprehensive program is helpful to healthcare of individuals with T2D. Of course, both drug and non-drug management of T2D require more solid evidence-based studies [
111].
Since there are more cardiovascular benefits in SGLT2 inhibitors, such as dapagliflozin [
112], and new animal models and clinical trials had already confirmed the glucose-lowering potential of glucokinase activators [
113], and there are more and better choices for T2D treatment, but we should pay more attention to both safety and efficacy of these novel hypoglycaemic drugs [
114]. Because T2D links to significant abnormalities in cardiocerebrovascular system [
115], such as atherosclerotic CVD, diabetic cardiomyopathy, CHF, stroke, CKD, peripheral neuropathy [
116], our program may have a role of risk-reduction of MACCE and improvement of clinical outcomes. Herein, this program can be adopted as “a concise guideline” in clinical practice due to OMT and healthy E(e)SEEDi lifestyle.
Both T2D (diagnosed and undiagnosed) and IGT are important CVD risk factors [
117] and have higher risk of coronary stenosis and coronary atherosclerotic plaques burden [
118]. When there is fragmented QRS, it may predict complex VAs and the risk of sudden cardiac death [
119], and LVDD is common [
120] in T2D patients, it may also be detected by 3D speckle tracking echocardiography [
121]. However, current SGLT2-inhibition remains to be at an underused status in these HF-population [
122]. A combination of agents high-intensity statins (rosuvastatin) and more often with ezetimibe [
123] and intensifying lifestyle measures is needed for stricter LDL-C and non-HDL-C targets.
Because good clinical investigations or programs could inform future diagnostic and therapeutic strategies, and enhance the understanding of a disease, just like myocardial infarction with nonobstructive coronary arteries (MINOCA) [
124] and this iRT-ABCDEFG program. When combined with novel tools [
125], new agents [
126], fresh preventive and interventional strategies [
127,
128], it will help us to get better effects on management or self-management of T2D. However, “advances in science are not linear, they are zigzag” [
129]. Thus, we should keep enough patience and confidence from papers publication to practical application and try to expand related clinical coverage.
During the pandemic and post-COVID-19 era [
130], both GLP-1 receptor agonists and SGLT2 inhibitors, when combined with the healthy E(e)SEEDi lifestyle, are effective in preventing related complications in T2D, such as CHF, CKD, and AF/AFL-reduction benefit. These medications have direct and favorable effects on protecting the heart and kidneys [
131,
132,
133,
134]. However, it should be noted that SGLT2 inhibitors do not have significant effects on ischemic events caused by atherosclerotic CVD in T2D [
135]. With the development of new drug delivery systems [
136,
137,
138] and technologies [
139,
140], there is potential for these medications to be even more effective in treating T2D and its complications.
As part of a healthy lifestyle, certain diets have been found to be beneficial in managing T2D. For example, the Mediterranean diet, which is rich in olive oil [
141], and avoids animal fats and refined carbohydrates can be helpful. Additionally, incorporating whole grains [
142], substituting yogurt or reduced-fat milk for cheese [
143], and supplementing with folate [
144] can also be beneficial. Consuming dietary fibers (DFs), particularly soluble fibers (SFs), from fruits [
145] and drinking green tea daily [
146] can also have a positive impact. Moderate alcohol consumption [
147], particularly wine, with meals [
148] and increased consumption of caffeinated coffee [
149] have also been linked to a lower risk of T2D. However, it is important to note that long-term consumption of artificially sweetened beverages (ASB), sugar-sweetened beverages (SSB), and total sweetened beverages (TSB) (a combination of ASB and SSB) have been associated with an increased risk of T2D [
150].
In addition, low birth weight and childhood obesity were associated with higher risk of adult T2D [
151]. No association of mushroom consumption with biomarkers and risks of CVD and T2D in US adults [
152], and not support an inverse association of yogurt consumption or other dairy consumption with T2D risk in black women [
153], no overall association between moderate egg consumption and risk of T2D [
154], But higher selenium concentration [
155], an adequate vitamin D status (around 50 nmol/L) and avoiding deficiency may help to prevent CVD complications among patients with T2D [
156].
New targets link to novel therapeutic strategies of T2D and its complications (CKD), such as the CCL25-CCR9 axis [
157], the IL-8-CXCR1/2 axis [
158], IL-6/glucagon [
159], Circulating ApoJ [
160], hydroxysteroid 17-beta dehydrogenase 6 (HSD17B6) [
161], and the gut microbiota [
162], and modification of lifestyles may reduce the risk of T2D, such as high adherence to a mainly plant-based diet [
163], improving cardiorespiratory fitness [
164], and the combination of antidiabetic agents and lifestyle [
165]. In addition, circulating miRNAs, particularly miR-486, miR-146b and miR-15b, are helpful in predicting the future risk of T2D [
166].
Since cases with T2D is easy to suffer from diabetic dyslipidaemia [
167] and dementia [
168], healthy lifestyle plays a vital role on lowering these risks. A series of studies showed that healthy lifestyles highly link to lower T2D risk, for example, foods of whole grains[
169], fruits, and dairy [
170], a more plant-based and less animal-based diet [
171], moderate wine consumption [
172] among overweight women, but lower levels of cognitive function [
173], sedentary behaviors (total sitting and TV viewing) [
174], foods of red meat, processed meat, and sugar-sweetened beverages [
170], and novel inflammatory markers (EN-RAGE, IL17, and IL13) [
175] link to high T2D risk. In fact, changes in body shape after puberty [
176], excess body weight [
177], and visceral adipose tissue [
178] may serve as an evaluating tool for prediction of T2D incidence. In a word, with the development of new pharmacotherapeutic approaches, novel therapeutic targets, and fresh lifestyle medicine, the up-to-date personalized therapeutic plan and program for T2D will be great helpful in the control and prevention of T2D.
6. Conclusions and Recommendations
This iRT-ABCDEFG program combining OMT and healthy E(e)SEEDi lifestyle for T2D is very suitable for healthcare among clinical doctors, patients, and healthy individuals. This program is helpful to access clinical vital goals, which include less MACCE and diabetic complications, less medical costs, longer life expectancy, lower morbidity and mortality, and higher quality of life due to early diagnosis, OMT, and overall prevention by healthy E(e)SEEDi lifestyle. Moreover, this program is not only effective but also not complicated, and easy to perform in primary care centers. In addition, training the professional members and individuals to carry out this program is so easy. In fact, this program can also be developed as a mobile APP for wide use among T2D individuals and general population. Herein, we highly recommend this iRT-ABCDEFG program due to a good expected cost-effective relationship and clinical outcomes, since T2D highly links to CVD (AMI, CHF, and stroke) and cancer, as well as other MACCE and the CDC strips.
Acknowledgments
The reviewers and editors are gratefully acknowledged for critical review.
Author Contributions
C.H. contributed to conceptualization, methodology, data curation, investigation, visualization, writing-original draft, writing-review & editing; T.T. contributed to conceptualization, data analysis, visualization, writing-review & editing; Q.W. contributed to conceptualization, data analysis, visualization, supervision, writing-review & editing. All the authors read and approved the final manuscript.
Ethics Statement
Not applicable.
Informed Consent Statement
Not applicable.
Funding
No funding for this study was received.
Declaration of Competing Interest
Dr. Tengiz Tkebuchava is affiliated with the company Boston TransTec, LLC, Boston, USA. The other authors have no disclosures to report.
References
1.
Lu J, Xia Q, Zhou Q. How to make insulin-producing pancreatic β cells for diabetes treatment.
Sci. China Life. Sci. 2017,
60, 239–248.
[Google Scholar]
2.
Lean MEJ, Leslie WS, Barnes AC, Brosnahan N, Thom G, McCombie L, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial.
Lancet 2018,
391, 541–551.
[Google Scholar]
3.
Mayer-Davis EJ, Lawrence JM, Dabelea D, Divers J, Isom S, Dolan L, et al. SEARCH for Diabetes in Youth Study. Incidence Trends of Type 1 and Type 2 Diabetes among Youths, 2002–2012.
N. Engl. J. Med. 2017,
376, 1419–1429.
[Google Scholar]
4.
Rawshani A, Rawshani A, Franzén S, Eliasson B, Svensson AM, Miftaraj M, et al. Mortality and Cardiovascular Disease in Type 1 and Type 2 Diabetes.
N. Engl. J. Med. 2017,
376, 1407–1418.
[Google Scholar]
5.
Lee C, Sung NJ, Lim HS, Lee JH. Emergency Department Visits Can Be Reduced by Having a Regular Doctor for Adults with Diabetes Mellitus: Secondary Analysis of 2013 Korea Health Panel Data.
J. Korean Med. Sci. 2017,
32, 1921–1930.
[Google Scholar]
6.
Kim MS, Lee DY. Urinary Glucose Screening for Early Detection of Asymptomatic Type 2 Diabetes in Jeonbuk Province Korean Schoolchildren.
J. Korean Med. Sci. 2017,
32, 985–991.
[Google Scholar]
7.
Shin WY, Lee T, Jeon DH, Kim HC. Diabetes, Frequency of Exercise, and Mortality Over 12 Years: Analysis of the National Health Insurance Service-Health Screening (NHIS-HEALS) Database.
J. Korean Med. Sci. 2018,
33, e60.
[Google Scholar]
8.
Cho S, Shin JY, Kim HJ, Eun SJ, Kang S, Jang WM, et al. Chasms in Achievement of Recommended Diabetes Care among Geographic Regions in Korea.
J. Korean Med. Sci. 2019,
34, e190.
[Google Scholar]
9.
Lloyd CE, Nouwen A, Sartorius N, Ahmed HU, Alvarez A, Bahendeka S, et al. Prevalence and correlates of depressive disorders in people with Type 2 diabetes: Results from the International Prevalence and Treatment of Diabetes and Depression (INTERPRET-DD) study, a collaborative study carried out in 14 countries.
Diabet. Med. 2018,
35, 760–769.
[Google Scholar]
10.
Wang JL, Qin Z, Wang ZJ, Shi DM, Liu YY, Zhao YX, et al. New predictors of in-stent restenosis in patients withdiabetes mellitusundergoing percutaneous coronary intervention with drug-eluting stent.
J. Geriatr. Cardiol. 2018,
15, 137–145.
[Google Scholar]
11.
Jakobsen GS, Småstuen MC, Sandbu R, Nordstrand N, Hofsø D, Lindberg M, et al. Association of Bariatric Surgery vs Medical Obesity Treatment with Long-term Medical Complications and Obesity-Related Comorbidities.
JAMA 2018,
319, 291–301.
[Google Scholar]
12.
Hu CS, Han YL, Ge JB, Wu QH, Liu YN, Ma CS, et al. A novel management program for hypertension.
Cardiovasc. Diagn. Ther. 2015,
5, 316–322.
[Google Scholar]
13.
Hu C, Tkebuchava T, Hu D. Managing acute myocardial infarction in China.
Eur. Heart J. 2019,
40, 1179–1181.
[Google Scholar]
14.
Hu CS, Wu QH, Hu DY, Tkebuchava T. Treatment of chronic heart failure in the 21st century: A new era of biomedical engineering has come.
Chronic Dis. Transl. Med. 2019,
5, 75–88.
[Google Scholar]
15.
Hu CS. A comprehensive strategy for managing arrhythmogenic right ventricular cardiomyopathy.
Turk. Kardiyol. Dern. Ars. 2020,
48, 88–95.
[Google Scholar]
16.
Hu CS. Intervention of RT-ABCDEF for cancer.
Croat. Med. J. 2019,
60, 55–57.
[Google Scholar]
17.
Hu CS, Tkebuchava T. SARS and its treatment strategies.
Asian Pac. J. Trop. Med. 2019,
12, 95–97.
[Google Scholar]
18.
Reaven PD, Emanuele NV, Wiitala WL, Bahn GD, Reda DJ, McCarren M, et al. VADT Investigators. Intensive Glucose Control in Patients with Type 2 Diabetes—15-Year Follow-up.
N. Engl. J. Med. 2019,
380, 2215–2224.
[Google Scholar]
19.
Schauer PR, Bhatt DL, Kirwan JP, Wolski K, Aminian A, Brethauer SA, et al. STAMPEDE Investigators. Bariatric Surgery versus Intensive Medical Therapy for Diabetes—5-Year Outcomes.
N. Engl. J. Med. 2017,
376, 641–651.
[Google Scholar]
20.
Gong L, Li R, Ren W, Wang Z, Wang Z, Yang M, et al. The FOXO1 Gene-Obesity Interaction Increases the Risk of Type 2 Diabetes Mellitus in a Chinese Han Population.
J. Korean Med. Sci. 2017,
32, 264–271.
[Google Scholar]
21.
Selvin E, Wang D, Lee AK, Bergenstal RM, Coresh J. Identifying Trends in Undiagnosed Diabetes in U.S. Adults by Using a Confirmatory Definition: A Cross-sectional Study.
Ann. Intern. Med. 2017,
167, 769–776.
[Google Scholar]
22.
Esteghamati A, Khandan A, Momeni A, Behdadnia A, Ghajar A, Nikdad MS, et al. Circulating levels of fibroblast growth factor 21 in early-stage diabetic kidney disease.
Ir. J. Med. Sci. 2017,
186, 785–794.
[Google Scholar]
23.
Liu B, Ye X, Zhao G, Jin L, Shi J. Association of RAGE with acute ischemic stroke prognosis in type 2 diabetes.
Ir. J. Med. Sci. 2021,
190, 625–630.
[Google Scholar]
24.
Argun D, Argun F, Borku Uysal B. Evaluation of salusin-alpha and salusin-beta levels in patients with type 2 diabetes mellitus and determination of the impact of severity of hyperglycemia on salusin levels.
Ir. J. Med. Sci. 2021,
190, 1403–1411.
[Google Scholar]
25.
Fangel MV, Nielsen PB, Kristensen JK, Larsen TB, Overvad TF, Lip GY, et al. Albuminuria and Risk of Cardiovascular Events and Mortality in a General Population of Patients with Type 2 Diabetes Without Cardiovascular Disease: A Danish Cohort Study.
Am. J. Med. 2020,
133, e269–e279.
[Google Scholar]
26.
Johansen MY, MacDonald CS, Hansen KB, Karstoft K, Christensen R, Pedersen M, et al.
Effect of an Intensive Lifestyle Intervention on Glycemic Control in Patients With Type 2 Diabetes A Randomized Clinical Trial.
JAMA 2017,
318, 637–646.
[Google Scholar]
27.
Hu C. Grants supporting research in China.
Eur. Heart J. 2018,
39, 2342–2344.
[Google Scholar]
28.
Hu CS, Tkebuchava T. SEEDi
1.0−3.0 strategies for major noncommunicable diseases in China.
J. Integr. Med. 2017,
15, 265–269.
[Google Scholar]
29.
Miller KA, Siscovick DS, Sheppard L, Shepherd K, Sullivan JH, Anderson GL, et al. Long-term exposure to air pollution and incidence of cardiovascular events in women.
N. Engl. J. Med. 2007,
356, 447–458.
[Google Scholar]
30.
Coogan PF, White LF, Jerrett M, Brook RD, Su JG, Seto E, et al. Air pollution and incidence of hypertension and diabetes mellitus in black women living in Los Angeles.
Circulation 2012,
125, 767–772.
[Google Scholar]
31.
Yang BY, Qian ZM, Li S, Chen G, Bloom MS, Elliott M, et al. Ambient air pollution in relation to diabetes and glucose-homoeostasis markers in China: A cross-sectional study with findings from the 33 Communities Chinese Health Study.
Lancet Planet. Health 2018,
2, e64–e73.
[Google Scholar]
32.
Bowe B, Xie Y, Li T, Yan Y, Xian H, Al-Aly Z. The 2016 global and national burden of diabetes mellitus attributable to PM(25) air pollution.
Lancet Planet. Health 2018,
2, e301–e312.
[Google Scholar]
33.
Zhang S, Mwiberi S, Pickford R, Breitner S, Huth C, Koenig W, et al. Longitudinal associations between ambient air pollution and insulin sensitivity: Results from the KORA cohort study.
Lancet Planet. Health 2021,
5, e39–e49.
[Google Scholar]
34.
Liu L, Wang F, Lu H, Cao S, Du Z, Wang Y, et al. Effects of Noise Exposure on Systemic and Tissue-Level Markers of Glucose Homeostasis and Insulin Resistance in Male Mice.
Environ. Health Perspect. 2016,
124, 1390–1398.
[Google Scholar]
35.
Hu CS, Tkebuchava T. E-noise: An increasingly relevant health risk.
J. Integr. Med. 2019,
17, 311–314.
[Google Scholar]
36.
Osborne MT, Naddaf N, Abohashem S, Radfar A, Ghoneem A, Dar T, Wang Y, et al. A neurobiological link between transportation noise exposure and metabolic disease in humans.
Psychoneuroendocrinology 2021,
131, 105331.
[Google Scholar]
37.
Eriksson JG, Kajantie E, Lampl M, Osmond C. Trajectories of body mass index amongst children who develop type 2 diabetes as adults.
J. Intern. Med. 2015,
278, 219–226.
[Google Scholar]
38.
Elmasry A, Lindberg E, Berne C, Janson C, Gislason T, Awad Tageldin M, et al. Sleep-disordered breathing and glucose metabolism in hypertensive men: A population-based study.
J. Intern. Med. 2001,
249, 153–161.
[Google Scholar]
39.
Pan KY, Xu W, Mangialasche F, Fratiglioni L, Wang HX. Work-related psychosocial stress and the risk of type 2 diabetes in later life.
J. Intern. Med. 2017,
281, 601–610.
[Google Scholar]
40.
Giovannucci EL, Rezende LFM, Lee DH. Muscle-strengthening activities and risk of cardiovascular disease, type 2 diabetes, cancer and mortality: A review of prospective cohort studies.
J. Intern. Med. 2021,
290, 789–805.
[Google Scholar]
41.
Wang Y, Lee DC, Brellenthin AG, Eijsvogels TMH, Sui X, Church TS, et al. Leisure-Time Running Reduces the Risk of Incident Type 2 Diabetes.
Am. J. Med. 2019,
132, 1225–1232.
[Google Scholar]
42.
Carlsson S, Andersson T, Araghi M, Galanti R, Lager A, Lundberg M, et al. Smokeless tobacco (snus) is associated with an increased risk of type 2 diabetes: Results from five pooled cohorts.
J. Intern. Med. 2017,
281, 398–406.
[Google Scholar]
43.
Shi L, Brunius C, Johansson I, Bergdahl IA, Rolandsson O, van Guelpen B, et al. Plasma metabolite biomarkers of boiled and filtered coffee intake and their association with type 2 diabetes risk.
J. Intern. Med. 2020,
287, 405–421.
[Google Scholar]
44.
Martin WP, Sharif F, Flaherty G. Lifestyle risk factors for cardiovascular disease and diabetic risk in a sedentary occupational group: The Galway taxi driver study.
Ir. J. Med. Sci. 2016,
185, 403–412.
[Google Scholar]
45.
Liu G, Li Y, Hu Y, Zong G, Li S, Rimm EB, et al. Influence of Lifestyle on Incident Cardiovascular Disease and Mortality in Patients with Diabetes Mellitus.
J. Am. Coll. Cardiol. 2018,
71, 2867–2876.
[Google Scholar]
46.
Newman JD, Schwartzbard AZ, Weintraub HS, Goldberg IJ, Berger JS. Primary Prevention of Cardiovascular Disease in Diabetes Mellitus.
J. Am. Coll. Cardiol. 2017,
70, 883–893.
[Google Scholar]
47.
Unick JL, Beavers D, Bond DS, Clark JM, Jakicic JM, Kitabchi AE, et al. Look AHEAD Research Group. The long-term effectiveness of a lifestyle intervention in severely obese individuals.
Am. J. Med. 2013,
126, 236–242.e1–e2.
[Google Scholar]
48.
Grabovac I, Smith L, Stefanac S, Haider S, Cao C, Waldhoer T, et al. Health Care Providers’ Advice on Lifestyle Modification in the US Population: Results from the NHANES 2011–2016.
Am. J. Med. 2019,
132, 489–497.e1.
[Google Scholar]
49.
Song G, Chen C, Zhang J, Chang L, Zhu D, Wang X. Association of traditional Chinese exercises with glycemic responses in people with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials.
J. Sport Health Sci. 2018,
7, 442–452.
[Google Scholar]
50.
McMacken M, Shah S. A plant-based diet for the prevention and treatment of type 2diabetes.
J. Geriatr. Cardiol. 2017,
14, 342–354.
[Google Scholar]
51.
ASCEND Study Collaborative Group, Bowman L, Mafham M, Wallendszus K, Stevens W, Buck G, Barton J, et al. Effects of n-3 Fatty Acid Supplements in Diabetes Mellitus.
N. Engl. J. Med. 2018,
379, 1540–1550.
[Google Scholar]
52.
Pittas AG, Dawson-Hughes B, Sheehan P, Ware JH, Knowler WC, Aroda VR, et al. D2d Research Group. Vitamin D Supplementation and Prevention of Type 2 Diabetes.
N. Engl. J. Med. 2019,
381, 520–530.
[Google Scholar]
53.
Hu CS, Tkebuchava T. New “P” in Medical Model.
Chin. Med. J. 2016,
129, 492–493..
[Google Scholar]
54.
Gazzaruso C, Coppola A, Pujia A, Falcone C, Collaviti S, Fodaro M, et al. Erectile dysfunction as a predictor of asymptomatic coronary artery disease in elderly men with type 2diabetes.
J. Geriatr. Cardiol. 2016,
13, 552–556.
[Google Scholar]
55.
Gudbjartsson DF, Thorgeirsson G, Sulem P, Helgadottir A, Gylfason A, Saemundsdottir J, et al. Lipoprotein(a) Concentration and Risks of Cardiovascular Disease and Diabetes.
J. Am. Coll. Cardiol. 2019,
74, 2982–2994.
[Google Scholar]
56.
Rutter MK, Wahid ST, McComb JM, Marshall SM. Significance of silent ischemia and microalbuminuria in predicting coronary events in asymptomatic patients with type 2 diabetes.
J. Am. Coll. Cardiol. 2002,
40, 56–61.
[Google Scholar]
57.
Low Wang CC, Blomster JI, Heizer G, Berger JS, Baumgartner I, Fowkes FGR, et al. EUCLID Trial Executive Committee and Investigators. Cardiovascular and Limb Outcomes in Patients With Diabetes and Peripheral Artery Disease: The EUCLID Trial.
J. Am. Coll. Cardiol. 2018,
72, 3274–3284.
[Google Scholar]
58.
Laiteerapong N, Cooper JM, Skandari MR, Clarke PM, Winn AN, Naylor RN, et al. Individualized Glycemic Control for U.S. Adults with Type 2 Diabetes: A Cost-Effectiveness Analysis.
Ann. Intern. Med. 2018,
168, 170–178.
[Google Scholar]
59.
Husain M, Birkenfeld AL, Donsmark M, Dungan K, Eliaschewitz FG, Franco DR, et al. PIONEER 6 Investigators. Oral Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes.
N. Engl. J. Med. 2019,
381, 841–851.
[Google Scholar]
60.
Tamborlane WV, Barrientos-Pérez M, Fainberg U, Frimer-Larsen H, Hafez M, Hale PM, et al. Ellipse Trial Investigators. Liraglutide in Children and Adolescents with Type 2 Diabetes.
N. Engl. J. Med. 2019,
381, 637–646.
[Google Scholar]
61.
Marso SP, Baeres FMM, Bain SC, Goldman B, Husain M, Nauck MA, et al. LEADER Trial Investigators. Effects of Liraglutide on Cardiovascular Outcomes in Patients With Diabetes With or Without Heart Failure.
J. Am. Coll. Cardiol. 2020,
75, 1128–1141.
[Google Scholar]
62.
Mann JFE, Ørsted DD, Brown-Frandsen K, Marso SP, Poulter NR, Rasmussen S, et al. LEADER Steering Committee and Investigators. Liraglutide and Renal Outcomes in Type 2 Diabetes.
N. Engl. J. Med. 2017,
377, 839–848.
[Google Scholar]
63.
Kosiborod M, Lam CSP, Kohsaka S, Kim DJ, Karasik A, Shaw J, et al. CVD-REAL Investigators and Study Group. Cardiovascular Events Associated With SGLT-2 Inhibitors Versus Other Glucose-Lowering Drugs: The CVD-REAL 2 Study.
J. Am. Coll. Cardiol. 2018,
71, 2628–2639.
[Google Scholar]
64.
Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, et al. CANVAS Program Collaborative Group. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes.
N. Engl. J. Med. 2017,
377, 644–657.
[Google Scholar]
65.
Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, et al. CREDENCE Trial Investigators. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy.
N. Engl. J. Med. 2019,
380, 2295–2306.
[Google Scholar]
66.
Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, et al. EMPA-REG OUTCOME Investigators. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes.
N. Engl. J. Med. 2016,
375, 323–334.
[Google Scholar]
67.
Sharma A, Ofstad AP, Ahmad T, Zinman B, Zwiener I, Fitchett D, et al. Patient Phenotypes and SGLT-2 Inhibition in Type 2 Diabetes: Insights From the EMPA-REG OUTCOME Trial.
JACC. Heart Fail. 2021,
9, 568–577.
[Google Scholar]
68.
Bilgin S, Kurtkulagi O, Duman TT, Tel BMA, Kahveci G, Kiran M, et al. Sodium glucose co-transporter-2 inhibitor, Empagliflozin, is associated with significant reduction in weight, body mass index, fasting glucose, and A1c levels in Type 2 diabetic patients with established coronary heart disease: The SUPER GATE study.
Ir. J. Med. Sci. 2021,
191, 1647–1652.
[Google Scholar]
69.
Marso SP, McGuire DK, Zinman B, Poulter NR, Emerson SS, Pieber TR, et al. DEVOTE Study Group. Efficacy and Safety of Degludec versus Glargine in Type 2 Diabetes.
N. Engl. J. Med. 2017,
377, 723–732.
[Google Scholar]
70.
Schmedt N, Enders D, Walker J, Garbe E, Douros A. Sodium-Glucose Co-Transporter 2 Inhibitors and the Risk of Venous Thromboembolism in Patients with Type 2 Diabetes: A Cohort Study.
Am. J. Med. 2021,
134, 606–613.e6.
[Google Scholar]
71.
Ferraro RA, Nass CM, Dudum R, Blumenthal RS, Sarkar S. What Clinicians Need to Know about the Cardiovascular Effects of the Most Recent Classes of Drugs Used for Type 2 Diabetes.
Am. J. Med. 2019,
132, 1027–1031.
[Google Scholar]
72.
Newman JD, Vani AK, Aleman JO, Weintraub HS, Berger JS, Schwartzbard AZ. The Changing Landscape of Diabetes Therapy for Cardiovascular Risk Reduction: JACC State-of-the-Art Review.
J. Am. Coll. Cardiol. 2018,
72, 1856–1869.
[Google Scholar]
73.
Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. DECLARE–TIMI 58 Investigators. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes.
N. Engl. J. Med. 2019,
380, 347–357.
[Google Scholar]
74.
Filippatos G, Bakris GL, Pitt B, Agarwal R, Rossing P, Ruilope LM, et al. FIDELIO-DKD Investigators. Finerenone Reduces New-Onset Atrial Fibrillation in Patients With Chronic Kidney Disease and Type 2 Diabetes.
J. Am. Coll. Cardiol. 2021,
78, 142–152.
[Google Scholar]
75.
Tan SY, Cronin H, Byrne S, O’Donovan A, Tuthill A. Appropriateness of aspirin prescribing for primary and secondary prevention of cardiovascular disease in type 2 diabetes in different care settings.
Ir. J. Med. Sci. 2022,
191, 1185–1191.
[Google Scholar]
76.
Liao EP. Patterns of medication initiation in newly diagnosed diabetes mellitus: Quality and cost implications.
Am. J. Med. 2012,
125, S1–S2.
[Google Scholar]
77.
Rana JS, Liu JY, Moffet HH, Sanchez RJ, Khan I, Karter AJ. Risk of Cardiovascular Events in Patients with Type 2 Diabetes and Metabolic Dyslipidemia Without Prevalent Atherosclerotic Cardiovascular Disease.
Am. J. Med. 2020,
133, 200–206.
[Google Scholar]
78.
Lavie G, Hoshen M, Leibowitz M, Benis A, Akriv A, Balicer R, et al. Statin Therapy for Primary Prevention in the Elderly and Its Association with New-Onset Diabetes, Cardiovascular Events, and All-Cause Mortality.
Am. J. Med. 2021,
134, 643–652.
[Google Scholar]
79.
Echouffo-Tcheugui JB, Xu H, Matsouaka RA, Xian Y, Schwamm LH, Smith EE, et al. Diabetes and long-term outcomes of ischaemic stroke: Findings from Get With The Guidelines-Stroke.
Eur. Heart J. 2018,
39, 2376–2386.
[Google Scholar]
80.
Atlas Writing Group, Timmis A, Townsend N, Gale C, Grobbee R, Maniadakis N, Flather M, et al. European Society of Cardiology: Cardiovascular Disease Statistics 2017.
Eur. Heart J. 2018,
39, 508–579.
[Google Scholar]
81.
Weng J, Zhou Z, Guo L, Zhu D, Ji L, Luo X, et al. T1D China Study Group. Incidence of type 1 diabetes in China, 2010–2013: Population based study.
BMJ 2018,
360, j5295.
[Google Scholar]
82.
Dieleman JL, Squires E, Bui AL, Campbell M, Chapin A, Hamavid H, et al. Factors Associated With Increases in US Health Care Spending, 1996–2013.
JAMA 2017,
318, 1668–1678.
[Google Scholar]
83.
Hu C, Tkebuchava T. Health in All Laws: A better strategy for global health.
J. Evid. Based. Med. 2022,
15, 10–14.
[Google Scholar]
84.
Hu CS, Tkebuchava T. Structure-Editing: A New Branch?
Chin. Med. J. 2016,
129, 1629–1630.
[Google Scholar]
85.
Halberg IB, Lyby K, Wassermann K, Heise T, Zijlstra E, Plum-Mörschel L. Efficacy and safety of oral basal insulin versus subcutaneous insulin glargine in type 2 diabetes: A randomised, double-blind, phase 2 trial.
Lancet Diabetes Endocrinol. 2019,
7, 179–188.
[Google Scholar]
86.
Ruiz HH, López Díez R, Arivazahagan L, Ramasamy R, Schmidt AM. Metabolism, Obesity, and Diabetes Mellitus.
Arterioscler. Thromb. Vasc. Biol. 2019,
39, e166–e174.
[Google Scholar]
87.
Chung MK, Eckhardt LL, Chen LY, Ahmed HM, Gopinathannair R, Joglar JA, et al. American Heart Association Electrocardiography and Arrhythmias Committee and Exercise, Cardiac Rehabilitation, and Secondary Prevention Committee of the Council on Clinical Cardiology; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular and Stroke Nursing; and Council on Lifestyle and Cardiometabolic Health Lifestyle and Risk Factor Modification for Reduction of Atrial Fibrillation: A Scientific Statement From the American Heart Association.
Circulation 2020,
141, e750–e772.
[Google Scholar]
88.
Rangaswami J, Bhalla V, de Boer IH, Staruschenko A, Sharp JA, Singh RR, et al. American Heart Association Council on the Kidney in Cardiovascular Disease; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Council on Lifestyle and Cardiometabolic Health Cardiorenal Protection with the Newer Antidiabetic Agents in Patients With Diabetes and Chronic Kidney Disease: A Scientific Statement From the American Heart Association.
Circulation 2020,
142, e265–e286.
[Google Scholar]
89.
Filippatos G, Anker SD, Agarwal R, Pitt B, Ruilope LM, Rossing P, et al. FIDELIO-DKD Investigators. Finerenone and Cardiovascular Outcomes in Patients with Chronic Kidney Disease and Type 2 Diabetes.
Circulation 2021,
143, 540–552.
[Google Scholar]
90.
The Lancet. Modernising the NHS: Leading the way with diabetes.
Lancet 2019,
393, 200.
[Google Scholar]
91.
Hu CS. Analysis of COVID-19 Cases and Public Measures in China.
SN Compr. Clin. Med. 2020,
2, 1306–1312.
[Google Scholar]
92.
Qian F, Liu G, Hu FB, Bhupathiraju SN, Sun Q. Association Between Plant-Based Dietary Patterns and Risk of Type 2 Diabetes: A Systematic Review and Meta-analysis.
JAMA. Intern. Med. 2019,
179, 1335–1344.
[Google Scholar]
93.
Owens-Gary MD, Zhang X, Jawanda S, Bullard KM, Allweiss P, Smith BD. The Importance of Addressing Depression and Diabetes Distress in Adults withType 2 Diabetes.
J. Gen. Intern. Med. 2019,
34, 320–324.
[Google Scholar]
94.
Vergari E, Denwood G, Salehi A, Zhang Q, Adam J, Alrifaiy A, et al. Somatostatin secretion by Na(+)-dependent Ca(2+)-induced Ca(2+) release in pancreatic delta-cells.
Nat. Metab. 2020,
2, 32–40.
[Google Scholar]
95.
De Jesus DF, Zhang Z, Kahraman S, Brown NK, Chen M, Hu J, et al. m(6)A mRNA Methylation Regulates Human β-Cell Biology in Physiological States and in Type 2 Diabetes.
Nat. Metab. 2019,
1, 765–774.
[Google Scholar]
96.
Campbell MD, Sathish T, Zimmet PZ, Thankappan KR, Oldenburg B, Owens DR, et al. Benefit of lifestyle-based T2DM prevention is influenced by prediabetes phenotype.
Nat. Rev. Endocrino. 2020,
16, 395–400.
[Google Scholar]
97.
Magkos F, Hjorth MF, Astrup A. Diet and exercise in the prevention and treatment of type 2 diabetes mellitus.
Nat. Rev. Endocrinol. 2020,
16, 545–555.
[Google Scholar]
98.
Perreault L, Skyler JS, Rosenstock J. Novel therapies with precision mechanisms for type 2 diabetes mellitus.
Nat. Rev. Endocrinol. 2021,
17, 364–377.
[Google Scholar]
99.
Caputo V, Termine A, Strafella C, Giardina E, Cascella R. Shared (epi)genomic background connecting neurodegenerative diseases and type 2 diabetes.
World J. Diabetes 2020,
11, 155–164.
[Google Scholar]
100.
Foran E, Hannigan A, Glynn L. Prevalence of depression in patients with type 2 diabetes mellitus in Irish primary care and the impact of depression on the control of diabetes.
Ir. J. Med. Sci. 2015,
184, 319–322.
[Google Scholar]
101.
Tudor RM, Garrahy A, Woods CP, Crowley RK, Tormey WT, Smith D, et al. The prevalence and incidence of thyroid dysfunction in patients with diabetes—A longitudinal follow-up study.
Ir. J. Med. Sci. 2020,
189, 171–175.
[Google Scholar]
102.
Manfrini O, Russo V, Ciavarella A, Ceroni L, Montalti M, Fattori R. Coronary plaque quantification and composition in asymptomatic patients with type II diabetes mellitus.
J. Cardiovasc. Med. 2012,
13, 423–431.
[Google Scholar]
103.
Stoynev N, Dimova I, Rukova B, Hadjidekova S, Nikolova D, Toncheva D, et al. Gene expression in peripheral blood of patients with hypertension and patients with type 2 diabetes.
J. Cardiovasc. Med. 2014,
15, 702–709.
[Google Scholar]
104.
Ruocco G, Evangelista I, Franci B, Lucani B, Martini S, Nuti R, et al. Combination of ST2 and B-type natriuretic peptide in diabetic patients with acute heart failure: Relation with ventricular stiffness and outcome.
J. Cardiovasc. Med. 2019,
20, 81–90.
[Google Scholar]
105.
De Luca G, Verdoia M, Savonitto S, Piatti L, Grosseto D, Morici N, et al. Elderly ACS 2 Investigators. Impact of diabetes on clinical outcome among elderly patients with acute coronary syndrome treated with percutaneous coronary intervention: Insights from the ELDERLY ACS 2 trial.
J. Cardiovasc. Med. 2020,
21, 453–459.
[Google Scholar]
106.
Zwart K, Velthuis S, Polyukhovych YV, Mosterd A, Smidt L, Serné EH, et al. Sodium-glucose cotransporter 2 inhibitors: A practical guide for the Dutch cardiologist based on real-world experience.
Neth. Heart J. 2021,
29, 490–499.
[Google Scholar]
107.
Pandey A, Vaduganathan M, Patel KV, Ayers C, Ballantyne CM, Kosiborod MN, et al. Biomarker-Based Risk Prediction of Incident Heart Failure in Pre-Diabetes and Diabetes.
JACC Heart Fail. 2021,
9, 215–223.
[Google Scholar]
108.
Echouffo-Tcheugui JB, Zhang S, Florido R, Hamo C, Pankow JS, Michos ED, et al. Duration of Diabetes and Incident Heart Failure: The ARIC (Atherosclerosis Risk In Communities) Study.
JACC Heart Fail. 2021,
9, 594–603.
[Google Scholar]
109.
Brandt-Jacobsen NH, Lav Madsen P, Johansen ML, Rasmussen JJ, Forman JL, Holm MR, et al. Mineralocorticoid Receptor Antagonist Improves Cardiac Structure in Type 2 Diabetes: Data From the MIRAD Trial.
JACC Heart Fail. 2021,
9, 550–558.
[Google Scholar]
110.
Pitt B, Filippatos G, Agarwal R, Anker SD, Bakris GL, Rossing P, et al. FIGARO-DKD Investigators. Cardiovascular Events with Finerenone in Kidney Disease and Type 2 Diabetes.
N. Engl. J. Med. 2021,
385, 2252–2263.
[Google Scholar]
111.
Hou L, Ge L, Li Y, Chen Y, Li H, He J, et al. Physical activity recommendations for patients with type2diabetes: A cross-sectional survey.
Acta Diabetol. 2020,
57, 765–777.
[Google Scholar]
112.
Phrommintikul A, Wongcharoen W, Kumfu S, Jaiwongkam T, Gunaparn S, Chattipakorn S, et al. Effects of dapagliflozin vs vildagliptin on cardiometabolic parameters in diabetic patients with coronary artery disease: A randomised study.
Br. J. Clin. Pharmacol. 2019,
85, 1337–1347.
[Google Scholar]
113.
Baker DJ, Wilkinson GP, Atkinson AM, Jones HB, Coghlan M, Charles AD, et al. Chronic glucokinase activator treatment at clinically translatable exposures gives durable glucose lowering in two animal models of type 2 diabetes.
Br. J. Pharmacol. 2014,
171, 1642–1654.
[Google Scholar]
114.
Shimazawa R, Ikeda M. Approvals of type 2 diabetes drugs tested in cardiovascular outcome trials: A tripartite comparison.
Br. J. Clin. Pharmacol. 2021,
87, 3938–3948.
[Google Scholar]
115.
Levelt E, Pavlides M, Banerjee R, Mahmod M, Kelly C, Sellwood J, et al. Ectopic and Visceral Fat Deposition in Lean and Obese Patients With Type 2 Diabetes.
J. Am. Coll. Cardiol. 2016,
68, 53–63.
[Google Scholar]
116.
Das SR, Everett BM, Birtcher KK, Brown JM, Cefalu WT, Januzzi JL Jr, et al. 2018 ACC Expert Consensus Decision Pathway on Novel Therapies for Cardiovascular Risk Reduction in Patients With Type 2 Diabetes and Atherosclerotic Cardiovascular Disease: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways.
J. Am. Coll. Cardiol. 2018,
72, 3200–3223.
[Google Scholar]
117.
Enquobahrie DA, Dolidze N, Chapidze G, Vadachkoria S, Soh J, Fitzpatrick A, et al. Type 2 diabetes and impaired glucose tolerance among cardiac patients.
Acta Cardiol. 2007,
62, 439–444.
[Google Scholar]
118.
Canpolat U, Aytemir K, Yorgun H, Hazirolan T, Kaya EB, Ateş AH, et al. Association of type 2 diabetes mellitus with coronary atherosclerotic plaque burden and morphology measured by multidetector computed tomography coronary angiography.
Acta Cardiol. 2012,
67, 71–77.
[Google Scholar]
119.
Eren H, Kaya Ü, Öcal L, Öcal AG, Genç Ö, Genç S, et al. Presence of fragmented QRS may be associated with complex ventricular arrhythmias in patients with type-2 diabetes mellitus.
Acta Cardiol. 2021,
76, 67–75.
[Google Scholar]
120.
Bayramoğlu A, Taşolar H, Kaya Y, Bektaş O, Kaya A, Yaman M, et al. Fragmented QRS complexes are associated with left ventricular dysfunction in patients with type-2 diabetes mellitus: A two-dimensional speckle tracking echocardiography study.
Acta Cardiol. 2018,
73, 449–456.
[Google Scholar]
121.
Wang Q, Fu C, Xia H, Gao Y. Aggravating effect of obstructive sleep apnoea on left ventricular remodelling and function disorder in patients with type 2 diabetes mellitus: A case-control study by 3D speckle tracking echocardiography.
Acta Cardiol. 2022,
77, 734–743.
[Google Scholar]
122.
Martens P, Janssens J, Ramaekers J, Dupont M, Mullens W. Contemporary choice of glucose lowering agents in heart failure patients with type 2 diabetes.
Acta Cardiol. 2020,
75, 211–217.
[Google Scholar]
123.
Hermans MP, Ahn SA, Rousseau MF. Lipid and cardiometabolic features of T2DM patients achieving stricter LDL-C and non-HDL-C targets in accordance with ESC/EAS 2019 guidelines.
Acta Cardiol. 2021,
76, 375–383.
[Google Scholar]
124.
Serpytis R, Majauskiene E, Navickas P, Lizaitis M, Glaveckaite S, Rucinskas K, et al. Randomized Pilot Trial on Optimal Treatment Strategy, Myocardial Changes, and Prognosis of Patients with Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA).
Am. J. Med. 2022,
135, 103–109.
[Google Scholar]
125.
Rauh SP, Rutters F, van der Heijden AAWA, Luimes T, Alssema M, Heymans MW, et al. External Validation of a Tool Predicting 7-Year Risk of Developing Cardiovascular Disease, Type 2 Diabetes or Chronic Kidney Disease.
J. Gen. Intern. Med. 2018,
33, 182–188.
[Google Scholar]
126.
Alexander JT, Staab EM, Wan W, Franco M, Knitter A, Skandari MR, et al. Longer-term Benefits and Risks of Sodium-Glucose Cotransporter-2 Inhibitors in Type 2 Diabetes: A Systematic Review and Meta-analysis.
J. Gen. Intern. Med. 2022,
37, 439–448.
[Google Scholar]
127.
Raghavan S, Pachucki MC, Chang Y, Porneala B, Fox CS, Dupuis J, et al. Incident Type 2 Diabetes Risk is Influenced by Obesity and Diabetes in Social Contacts: A Social Network Analysis.
J. Gen. Intern. Med. 2016,
31, 1127–1133.
[Google Scholar]
128.
Kobe EA, Lewinski AA, Jeffreys AS, Smith VA, Coffman CJ, Danus SM, et al. Implementation of an Intensive Telehealth Intervention for Rural Patients with Clinic-Refractory Diabetes.
J. Gen. Intern. Med. 2022,
37, 3080–3088.
[Google Scholar]
129.
Alpert JS. Advances in Science Are Not Linear; They Are Zigzag.
Am. J. Med. 2022,
135, 543–544.
[Google Scholar]
130.
Anastasiou G, Hatziagelaki E, Liberopoulos E. Could Dapagliflozin Attenuate COVID-19 Progression in High-Risk Patients With or Without Diabetes? Behind DARE-19 Concept.
J. Cardiovasc. Pharmacol. 2021,
78, e12–e19.
[Google Scholar]
131.
Li W, Chen X, Xie X, Xu M, Xu L, Liu P, et al. Comparison of sodium-glucose co-transporter 2 inhibitors and glucagon-like peptide receptor agonists for atrial fibrillation in type 2 diabetes mellitus: Systematic review with network meta-analysis of randomised controlled trials.
J. Cardiovasc. Pharmacol. 2022,
79, 281–288.
[Google Scholar]
132.
Qiu M, Ding LL, Wei XB, Liu SY, Zhou HR. Comparative Efficacy of Glucagon-like Peptide 1 Receptor Agonists and Sodium Glucose Cotransporter 2 Inhibitors for Prevention of Major Adverse Cardiovascular Events in Type 2 Diabetes: A Network Meta-analysis.
J. Cardiovasc. Pharmacol. 2021,
77, 34–37.
[Google Scholar]
133.
Vider E, Sapir R, Mosseri E, Gavioli E. Current perspectives of the use of Sodium Glucose Transport-2 Inhibitors for patients with heart failure and chronic kidney disease.
J. Cardiovasc. Pharmacol. 2022,
79, 247–253.
[Google Scholar]
134.
Zheng RJ, Wang Y, Tang JN, Duan JY, Yuan MY, Zhang JY. Association of SGLT2 inhibitors with risk of atrial fibrillation and stroke in patients with and without type 2 diabetes: A systemic review and meta-analysis of randomized controlled trials.
J. Cardiovasc. Pharmacol. 2022,
79, e145–e152.
[Google Scholar]
135.
Ye G, Wang S, Peng D. Effects of SGLT2 Inhibitor on Ischemic Events Stemming From Atherosclerotic Coronary Diseases: A Systematic Review and Meta-analysis With Trial Sequential Analysis of Randomized Controlled Trials.
J. Cardiovasc. Pharmacol. 2021,
77, 787–795.
[Google Scholar]
136.
Wang Z, Guo W, Kuang X, Hou S, Liu H. Nanopreparations for mitochondria targeting drug delivery system: Current strategies and future prospective.
Asian J. Pharm. Sci. 2017,
12, 498–508.
[Google Scholar]
137.
Yang L, Yang Y, Chen H, Mei L, Zeng X. Polymeric microneedle-mediated sustained release systems: Design strategies and promising applications for drug delivery.
Asian J. Pharm. Sci. 2022,
17, 70–86.
[Google Scholar]
138.
Ng LC, Gupta M. Transdermal drug delivery systems in diabetes management: A review.
Asian J. Pharm. Sci. 2020,
15, 13–25.
[Google Scholar]
139.
Liu Y, Zhou S, Gao Y, Zhai Y. Electrospun nanofibers as a wound dressing for treating diabetic foot ulcer.
Asian J. Pharm. Sci. 2019,
14, 130–143.
[Google Scholar]
140.
Simos YV, Spyrou K, Patila M, Karouta N, Stamatis H, Gournis D, et al. Trends of nanotechnology in type 2 diabetes mellitus treatment.
Asian J. Pharm. Sci. 2021,
16, 62–76.
[Google Scholar]
141.
Gomez-Marin B, Gomez-Delgado F, Lopez-Moreno J, Alcala-Diaz JF, Jimenez-Lucena R, Torres-Peña JD, et al. Long-term consumption of a Mediterranean diet improves postprandial lipemia in patients with type 2 diabetes: The Cordioprev randomized trial.
Am. J. Clin. Nutr. 2018,
108, 963–970.
[Google Scholar]
142.
Ardisson Korat AV, Li Y, Sacks F, Rosner B, Willett WC, Hu FB, et al. Dairy fat intake and risk of type 2 diabetes in 3 cohorts of US men and women.
Am. J. Clin. Nutr. 2019,
110, 1192–1200.
[Google Scholar]
143.
Drouin-Chartier JP, Li Y, Ardisson Korat AV, Ding M, Lamarche B, Manson JE, et al. Changes in dairy product consumption and risk of type 2 diabetes: Results from 3 large prospective cohorts of US men and women.
Am. J. Clin. Nutr. 2019,
110, 1201–1212.
[Google Scholar]
144.
Lind MV, Lauritzen L, Kristensen M, Ross AB, Eriksen JN. Effect of folate supplementation on insulin sensitivity and type 2 diabetes: A meta-analysis of randomized controlled trials.
Am. J. Clin. Nutr. 2019,
109, 29–42.
[Google Scholar]
145.
Partula V, Deschasaux M, Druesne-Pecollo N, Latino-Martel P, Desmetz E, Chazelas E, et al. Associations between consumption of dietary fibers and the risk of cardiovascular diseases, cancers, type 2 diabetes, and mortality in the prospective NutriNet-Santé cohort.
Am. J. Clin. Nutr. 2020,
112, 195–207.
[Google Scholar]
146.
Nie J, Yu C, Guo Y, Pei P, Chen L, Pang Y, et al. Tea consumption and long-term risk of type 2 diabetes and diabetic complications: A cohort study of 0.5 million Chinese adults.
Am. J. Clin. Nutr. 2021,
114, 194–202.
[Google Scholar]
147.
Rose BD, Rimm EB, Zhang X, Sun Q, Huang T, Young RL, et al. You are What You Drink? How Associations Between Profiles of Beverage Consumption and Type 2 Diabetes Risk are Mediated by Biomarker Networks.
Am. J. Clin. Nutr. 2023,
118, 68–76.
[Google Scholar]
148.
Ma H, Wang X, Li X, Heianza Y, Qi L. Moderate alcohol drinking with meals is related to lower incidence of type 2 diabetes.
Am. J. Clin. Nutr. 2022,
116, 1507–1514.
[Google Scholar]
149.
Yang J, Tobias DK, Li S, Bhupathiraju SN, Ley SH, Hinkle SN, et al. Habitual coffee consumption and subsequent risk of type 2 diabetes in individuals with a history of gestational diabetes—a prospective study.
Am. J. Clin. Nutr. 2022,
116, 1693–1703.
[Google Scholar]
150.
Hirahatake KM, Jacobs DR, Shikany JM, Jiang L, Wong ND, Steffen LM, et al. Cumulative intake of artificially sweetened and sugar-sweetened beverages and risk of incident type 2 diabetes in young adults: The Coronary Artery Risk Development In Young Adults (CARDIA) Study.
Am. J. Clin. Nutr. 2019,
110, 733–741.
[Google Scholar]
151.
Wang W, Lv J, Yu C, Guo Y, Pei P, Zhuang Z, et al. China Kadoorie Biobank Collaborative Group. Lifestyle factors and fetal and childhood origins of type 2 diabetes: A prospective study of Chinese and European adults.
Am. J. Clin. Nutr. 2022,
115, 749–758.
[Google Scholar]
152.
Lee DH, Yang M, Giovannucci EL, Sun Q, Chavarro JE. Mushroom consumption, biomarkers, and risk of cardiovascular disease and type 2 diabetes: A prospective cohort study of US women and men.
Am. J. Clin. Nutr. 2019,
110, 666–674.
[Google Scholar]
153.
Rosenberg L, Robles YP, Li S, Ruiz-Narvaez EA, Palmer JR. A prospective study of yogurt and other dairy consumption in relation to incidence of type 2 diabetes among black women in the USA.
Am. J. Clin. Nutr. 2020,
112, 512–518.
[Google Scholar]
154.
Drouin-Chartier JP, Schwab AL, Chen S, Li Y, Sacks FM, Rosner B, et al. Egg consumption and risk of type 2 diabetes: Findings from 3 large US cohort studies of men and women and a systematic review and meta-analysis of prospective cohort studies.
Am. J. Clin. Nutr. 2020,
112, 619–630.
[Google Scholar]
155.
Qiu Z, Geng T, Wan Z, Lu Q, Guo J, Liu L, et al. Serum selenium concentrations and risk of all-cause and heart disease mortality among individuals with type 2 diabetes.
Am. J. Clin. Nutr. 2022,
115, 53–60.
[Google Scholar]
156.
Wan Z, Geng T, Li R, Chen X, Lu Q, Lin X, et al. Vitamin D status, genetic factors, and risks of cardiovascular disease among individuals with type 2 diabetes: A prospective study.
Am. J. Clin. Nutr. 2022,
116, 1389–1399.
[Google Scholar]
157.
Atanes P, Lee V, Huang GC, Persaud SJ. The role of the CCL25-CCR9 axis in beta-cell function: Potential for therapeutic intervention in type 2 diabetes.
Metabolism 2020,
113, 154394.
[Google Scholar]
158.
Loretelli C, Rocchio F, D’Addio F, Ben Nasr M, Castillo-Leon E, Dellepiane S, et al. The IL-8-CXCR1/2 axis contributes to diabetic kidney disease.
Metabolism 2021,
121, 154804.
[Google Scholar]
159.
Chen W, Cui W, Wu J, Zheng W, Sun X, Zhang J, et al. Blocking IL-6 signaling improves glucose tolerance via SLC39A5-mediated suppression of glucagon secretion.
Metabolism 2023,
146, 155641.
[Google Scholar]
160.
Seo JA, Kang MC, Ciaraldi TP, Kim SS, Park KS, Choe C, et al. Circulating ApoJ is closely associated with insulin resistance in human subjects.
Metabolism 2018,
78, 155–166.
[Google Scholar]
161.
Wei F, Gu Y, He L, Kapoor A, Lin X, Dong Y, et al. HSD17B6 delays type 2 diabetes development via inhibiting SREBP activation.
Metabolism 2023,
145, 155631.
[Google Scholar]
162.
Yang G, Wei J, Liu P, Zhang Q, Tian Y, Hou G, et al. Role of the gut microbiota in type 2 diabetes and related diseases.
Metabolism 2021,
117, 154712.
[Google Scholar]
163.
Zhang S, Stubbendorff A, Olsson K, Ericson U, Niu K, Qi L, et al. Adherence to the EAT-Lancet diet, genetic susceptibility, and risk of type 2 diabetes in Swedish adults.
Metabolism 2023,
141, 155401.
[Google Scholar]
164.
Xu C, Hou Y, Si K, Cao Z. Cardiorespiratory fitness, genetic susceptibility, inflammation and risk of incident type 2 diabetes: A population-based longitudinal study.
Metabolism 2022,
132, 155215.
[Google Scholar]
165.
Guardado-Mendoza R, Salazar-López SS, Álvarez-Canales M, Farfán-Vázquez D, Martínez-López YE, Jiménez-Ceja LM, et al. The combination of linagliptin, metformin and lifestyle modification to prevent type 2 diabetes (PRELLIM). A randomized clinical trial.
Metabolism 2020,
104, 154054.
[Google Scholar]
166.
Cui X, You L, Zhu L, Wang X, Zhou Y, Li Y, et al. Change in circulating microRNA profile of obese children indicates future risk of adult diabetes.
Metabolism 2018,
78, 95–105.
[Google Scholar]
167.
Neuenschwander M, Hoffmann G, Schwingshackl L, Schlesinger S. Impact of different dietary approaches on blood lipid control in patients with type 2 diabetes mellitus: A systematic review and network meta-analysis.
Eur. J. Epidemiol. 2019,
34, 837–852.
[Google Scholar]
168.
Lai HTM, Chang K, Sharabiani MTA, Valabhji J, Gregg EW, Middleton L, et al. Twenty-year trajectories of cardio-metabolic factors among people with type 2 diabetes by dementia status in England: A retrospective cohort study.
Eur. J. Epidemiol. 2023,
38, 733–744.
[Google Scholar]
169.
Parker ED, Liu S, Van Horn L, Tinker LF, Shikany JM, Eaton CB, et al. The association of whole grain consumption with incident type 2 diabetes: The Women’s Health Initiative Observational Study.
Ann. Epidemiol. 2013,
23, 321–327.
[Google Scholar]
170.
Schwingshackl L, Hoffmann G, Lampousi AM, Knüppel S, Iqbal K, Schwedhelm C, et al. Food groups and risk of type 2 diabetes mellitus: A systematic review and meta-analysis of prospective studies.
Eur. J. Epidemiol. 2017,
32, 363–375.
[Google Scholar]
171.
Chen Z, Zuurmond MG, van der Schaft N, Nano J, Wijnhoven HAH, Ikram MA, et al. Plant versus animal based diets and insulin resistance, prediabetes and type 2 diabetes: The Rotterdam Study.
Eur. J. Epidemiol. 2018,
33, 883–893.
[Google Scholar]
172.
Fagherazzi G, Vilier A, Lajous M, Boutron-Ruault MC, Balkau B, Clavel-Chapelon F, et al. Wine consumption throughout life is inversely associated with type 2 diabetes risk, but only in overweight individuals: Results from a large female French cohort study.
Eur. J. Epidemiol. 2014,
29, 831–839.
[Google Scholar]
173.
Bjerregaard LG, Damborg ML, Osler M, Sørensen TIA, Baker JL. Body mass index and height in relation to type 2 diabetes by levels of intelligence and education in a large cohort of Danish men.
Eur. J. Epidemiol. 2020,
35, 1167–1175.
[Google Scholar]
174.
Patterson R, McNamara E, Tainio M, de Sá TH, Smith AD, Sharp SJ, et al. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: A systematic review and dose response meta-analysis.
Eur. J. Epidemiol. 2018,
33, 811–829.
[Google Scholar]
175.
Brahimaj A, Ligthart S, Ghanbari M, Ikram MA, Hofman A, Franco OH, et al. Novel inflammatory markers for incident pre-diabetes and type 2 diabetes: The Rotterdam Study.
Eur. J. Epidemiol. 2017,
32, 217–226.
[Google Scholar]
176.
Fagherazzi G, Vilier A, Affret A, Balkau B, Bonnet F, Clavel-Chapelon F. The association of body shape trajectories over the life course with type 2 diabetes risk in adulthood: A group-based modeling approach.
Ann. Epidemiol. 2015,
25, 785–787.
[Google Scholar]
177.
Mehta N, Stenholm S, Männistö S, Jousilahti P, Elo I. Excess body weight, cigarette smoking, and type II diabetes incidence in the national FINRISK studies.
Ann. Epidemiol. 2020,
42, 12–18.
[Google Scholar]
178.
Maskarinec G, Raquinio PA, Setiawan VW, Ernst T, Franke AA, Buchthal SD, et al. Biomarker-based visceral adiposity score and incident type 2 diabetes in the multiethnic cohort.
Ann. Epidemiol. 2021,
63, 29–34.
[Google Scholar]